

Sarcopenia: Current treatments and new regenerative therapeutic approaches
- PMID: 32489859
- PMCID: PMC7256062
- DOI: 10.1016/j.jot.2020.04.002
Sarcopenia: Current treatments and new regenerative therapeutic approaches
Abstract
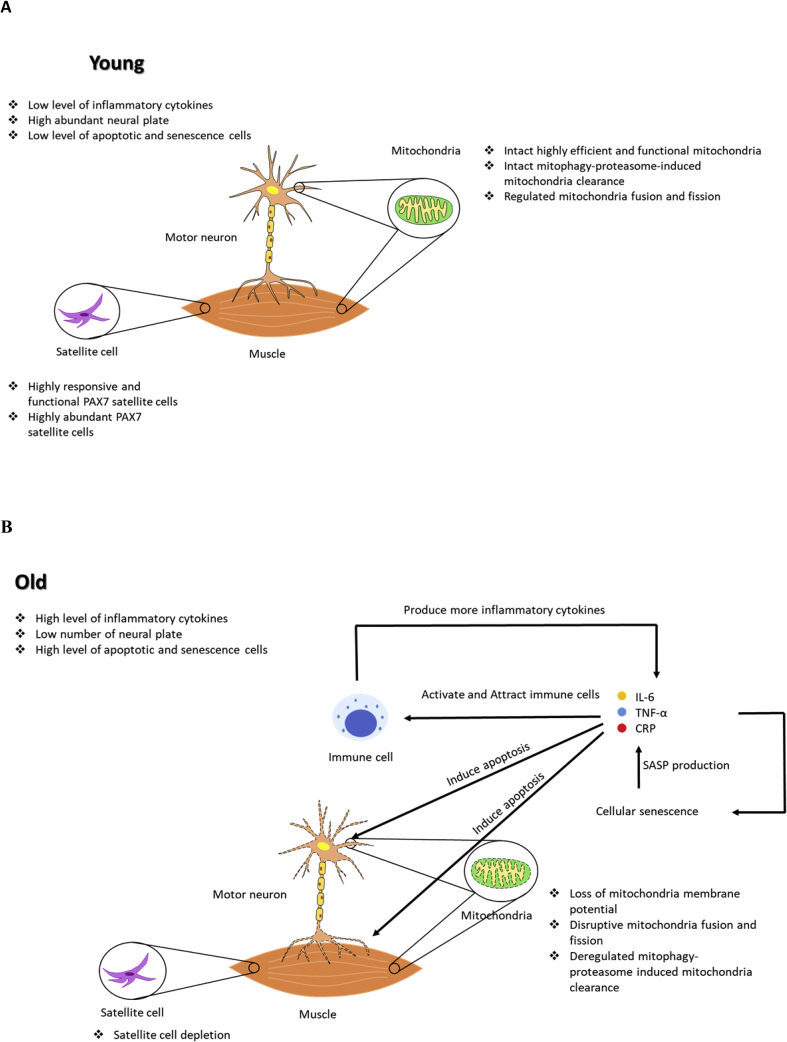
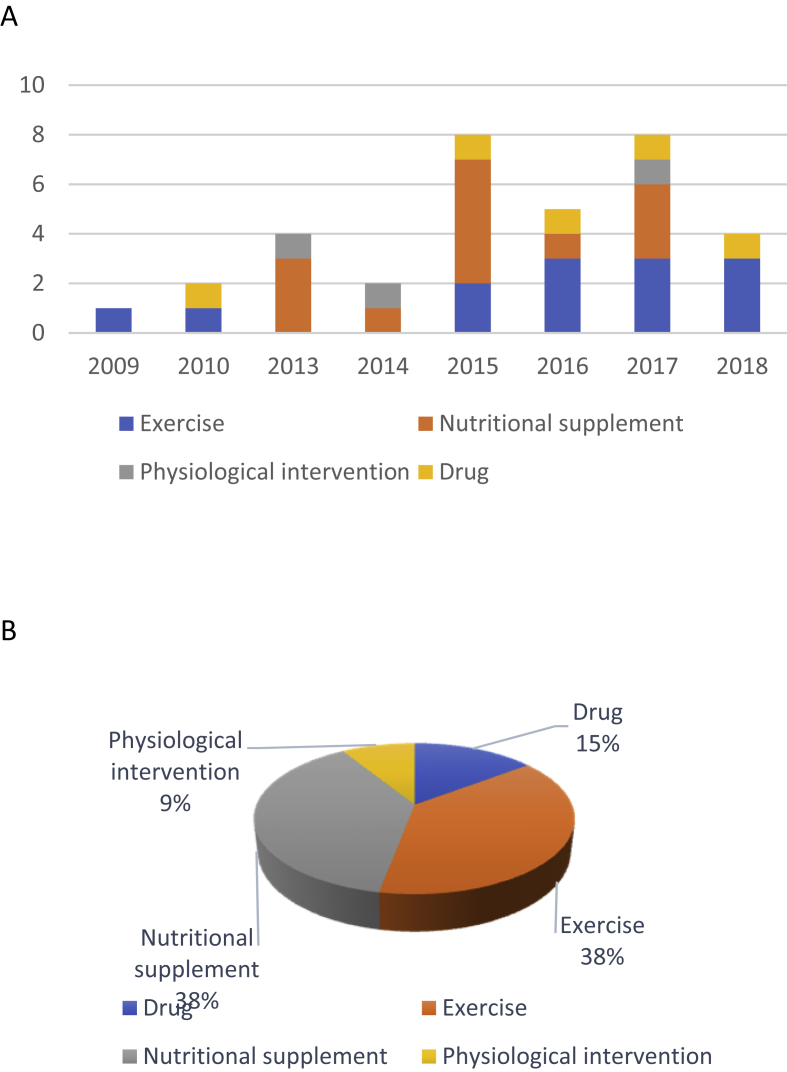
Sarcopenia is characterized by loss of muscle and reduction in muscle strength that contributes to higher mortality rate and increased incidence of fall and hospitalization in the elderly. Mitochondria dysfunction and age-associated inflammation in muscle are two of the main attributors to sarcopenia progression. Recent clinical trials on sarcopenia therapies such as physical exercise, nutraceutical, and pharmaceutical interventions have revealed that exercise is the only effective strategy shown to alleviate sarcopenia. Unlike nutraceutical and pharmaceutical interventions that showed controversial results in sarcopenia alleviation, exercise was found to restore mitochondria homeostasis and dampen inflammatory responses via a complex exchange of myokines and osteokines signalling between muscle and bone. However, as exercise have limited benefit to immobile patients, the use of stem cells and their secretome are being suggested to be novel therapeutics that can be catered to a larger patient population owing to their mitochondria restoration effects and immune modulatory abilities. As such, we reviewed the potential pros and cons associated with various stem cell types/secretome in sarcopenia treatment and the regulatory and production barriers that need to be overcome to translate such novel therapeutic agents into bedside application. Translational potential: This review summarizes the causes underlying sarcopenia from the perspective of mitochondria dysfunction and age-associated inflammation, and the progress of clinical trials for the treatment of sarcopenia. We also propose therapeutic potential of stem cell therapy and bioactive secretome for sarcopenia.
Keywords: Clinical trial; Exercise; Inflammation; Mesenchymal stem/stromal cells; Mitochondria; Sarcopenia.
© 2020 The Author(s).
Conflict of interest statement
The authors have no conflicts of interest to disclose in relation to this article.
Figures


References
-
- Beard J.R., Officer A.M., Cassels A.K. The World report on ageing and health. Gerontol. 2016;56(Suppl 2):S163–S166. - PubMed
-
- Lexell J., Taylor C.C., Sjostrom M. What is the cause of the ageing atrophy? Total number, size and proportion of different fiber types studied in whole vastus lateralis muscle from 15- to 83-year-old men. J Neurol Sci. 1988;84(2–3):275–294. - PubMed
-
- Rosenberg I.H. Sarcopenia: origins and clinical relevance. J Nutr. 1997;127(5 Suppl) 990S-1S. - PubMed
-
- Sayer A.A., Dennison E.M., Syddall H.E., Gilbody H.J., Phillips D.I., Cooper C. Type 2 diabetes, muscle strength, and impaired physical function: the tip of the iceberg? Diabetes Care. 2005;28(10):2541–2542. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
