

Comorbidities and their link with individual health status: A cross-sectional analysis of 23,892 people with knee and hip osteoarthritis from primary care
- PMID: 32489945
- PMCID: PMC7238776
- DOI: 10.1177/2235042X20920456
Comorbidities and their link with individual health status: A cross-sectional analysis of 23,892 people with knee and hip osteoarthritis from primary care
Abstract
Objectives: Robust data on the impact of comorbidities on health in people with osteoarthritis (OA) are lacking, despite its potential importance for patient management. Objectives were to determine coexisting conditions in people with OA in primary care and whether more comorbidities were linked with individual health status.
Methods: A retrospective analysis of 23,892 patients with knee and hip OA was conducted to determine comorbidities present (number/clusters) and how these linked with pain intensity (0-100), widespread pain (site numbers), medication usage (paracetamol, nonsteroidal anti-inflammatory drugs, opioids), quality of life EuroQol five dimension scale (EQ-5D), and physical function (walking speed) using independent t-tests or χ 2 test.
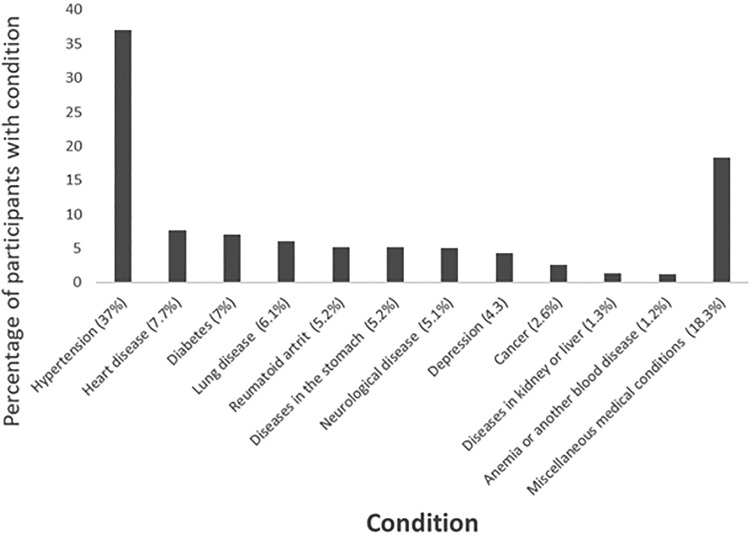
Results: Sixty-two percent of people with OA treated in primary care had at least one comorbidity; hypertension (37%), heart disease (8%), and diabetes (7%) being most common. Outcome measures worsened with more comorbidities (0-4+ comorbidities); pain intensity [mean (SD)] 46(22)-57(21); number of painful sites 3.7(3.0)-6.3(5.4); quality of life 0.73(0.10)-0.63(0.15); walking speed 1.57 m/s (0.33)-1.24 m/s (0.31), while the proportion of people using pain medication increased from 0 to 2 comorbidities (58-69%; p < 0.001), with an increase in opioid use from 4.6% to 19.5% with more comorbidities (0-4+ comorbidities).
Conclusion: Most people with knee or hip OA in primary care have at least one other long-term condition. A greater number of comorbidities is linked with worsening health, highlighting the importance of screening for comorbidities when treating patients with OA. It is important for clinicians to consider how OA treatments will interact and affect other common comorbidities.
Keywords: Osteoarthritis; comorbidity; health status; multimorbidity.
© The Author(s) 2020.
Conflict of interest statement
Declaration of conflicting interests: The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: EMR is the deputy editor of Osteoarthritis and Cartilage, the developer of the Knee injury and Osteoarthritis Outcome Score (KOOS) and several other freely available patient-reported outcome measures, and cofounder of Good Life with Osteoarthritis in Denmark (GLA: D®), a not-for-profit initiative hosted at the University of Southern Denmark aimed at implementing clinical guidelines for OA in clinical practice. STS, an associate editor of the Journal of Orthopaedic & Sports Physical Therapy, has received grants from The Lundbeck Foundation, personal fees from Munksgaard, all of which are outside the submitted work. He is the cofounder of GLA: D®.
Figures
References
-
- Farmer C, Fenu E, O’Flynn N, et al. Clinical assessment and management of multimorbidity: summary of NICE guidance. BMJ 2016; 354: 4843. - PubMed
-
- Barnett K, Mercer SW, Norbury M, et al. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet 2012; 380(9836): 37–43. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
