

Safety and Feasibility of Additional Tumor Debulking to First-Line Palliative Combination Chemotherapy for Patients with Multiorgan Metastatic Colorectal Cancer
- PMID: 32490570
- PMCID: PMC7418352
- DOI: 10.1634/theoncologist.2019-0693
Safety and Feasibility of Additional Tumor Debulking to First-Line Palliative Combination Chemotherapy for Patients with Multiorgan Metastatic Colorectal Cancer
Abstract
Introduction: Local treatment of metastases is frequently performed in patients with multiorgan metastatic colorectal carcinoma (mCRC) analogous to selected patients with oligometastatic disease for whom this is standard of care. The ORCHESTRA trial (NCT01792934) was designed to prospectively evaluate overall survival benefit from tumor debulking in addition to chemotherapy in patients with multiorgan mCRC. Here, we report the preplanned safety and feasibility evaluation after inclusion of the first 100 patients.
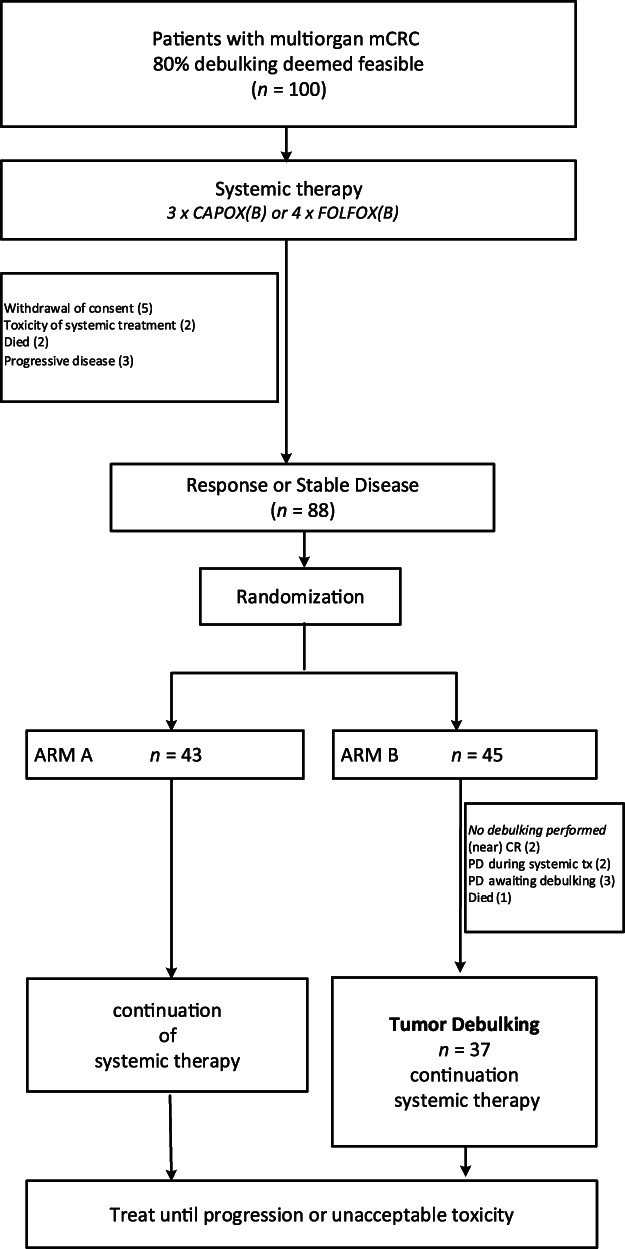
Methods: Patients were eligible if at least 80% tumor debulking was deemed feasible by resection, radiotherapy and/or thermal ablative therapy. In case of clinical benefit after three or four cycles of respectively 5-fluorouracil/leucovorin or capecitabine and oxaliplatin ± bevacizumab patients were randomized to tumor debulking followed by chemotherapy in the intervention arm, or standard treatment with chemotherapy.
Results: Twelve patients dropped out prior to randomization for various reasons. Eighty-eight patients were randomized to the standard (n = 43) or intervention arm (n = 45). No patients withdrew after randomization. Debulking was performed in 82% (n = 37). Two patients had no lesions left to treat, five had progressive disease, and one patient died prior to local treatment. In 15 patients (40%) 21 serious adverse events related to debulking were reported. Postoperative mortality was 2.7% (n = 1). After debulking chemotherapy was resumed in 89% of patients.
Conclusion: Tumor debulking is feasible and does not prohibit administration of palliative chemotherapy in the majority of patients with multiorgan mCRC, despite the occurrence of serious adverse events related to local treatment.
Implications for practice: This first prospective randomized trial on tumor debulking in addition to chemotherapy shows that local treatment of metastases is feasible in patients with multiorgan metastatic colorectal cancer and does not prohibit administration of palliative systemic therapy, despite the occurrence of serious adverse events related to local treatment. The trial continues accrual, and overall survival (OS) data and quality of life assessment are collected to determine whether the primary aim of >6 months OS benefit with preserved quality of life will be met. This will support evidence-based decision making in multidisciplinary colorectal cancer care and can be readily implemented in daily practice.
Keywords: Cytoreduction; Debulking; Metastatic colorectal cancer; Radiofrequency ablation; Stereotactic ablative radiotherapy.
© 2020 The Authors. The Oncologist published by Wiley Periodicals LLC on behalf of AlphaMed Press.
Conflict of interest statement
Figures
References
-
- Rees M, Tekkis PP, Welsh FK et al. Evaluation of long‐term survival after hepatic resection for metastatic colorectal cancer: A multifactorial model of 929 patients. Ann Surg 2008;247:125–135. - PubMed
-
- van der Pool AE, de Wilt JH, Lalmahomed ZS et al. Optimizing the outcome of surgery in patients with rectal cancer and synchronous liver metastases. Br J Surg 2010;97:383–390. - PubMed
-
- Tomlinson JS, Jarnagin WR, DeMatteo RP et al. Actual 10‐year survival after resection of colorectal liver metastases defines cure. J Clin Oncol 2007;25:4575–4580. - PubMed
-
- van der Pool AE, Mendez RA, Wunderink W et al. Stereotactic body radiation therapy for colorectal liver metastases. Br J Surg 2010;97:377–382. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
