

Understanding the age divide in COVID-19: why are children overwhelmingly spared?
- PMID: 32491949
- PMCID: PMC7324935
- DOI: 10.1152/ajplung.00183.2020
Understanding the age divide in COVID-19: why are children overwhelmingly spared?
Abstract
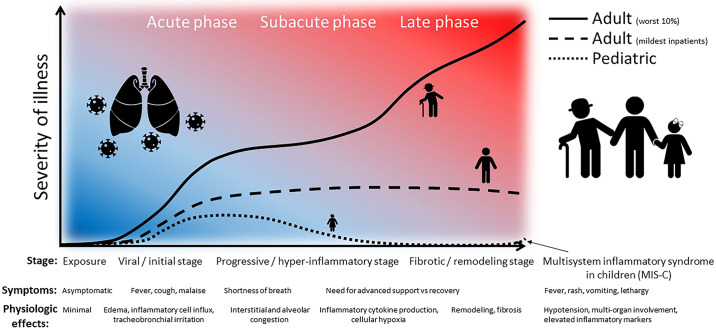
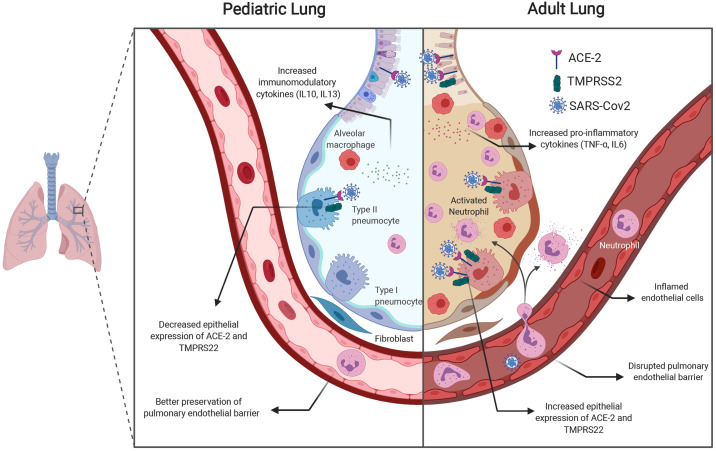
The rapid emergence and subsequent global dissemination of SARS-CoV-2 disease (COVID-19) has resulted in over 4 million cases worldwide. The disease has a marked predilection for adults, and children are relatively spared. Understanding the age-based differences in pathophysiological pathways and processes relevant to the onset and progression of disease both in the clinical course and in experimental disease models may hold the key to the identification of therapeutic targets. The differences in the clinical course are highlighted by the lack of progression of the SARS-CoV-2 infection beyond mild symptoms in a majority of children, whereas in adults the disease progresses to acute lung injury and an acute respiratory distress syndrome (ARDS)-like phenotype with high mortality. The pathophysiological mechanisms leading to decreased lung injury in children may involve the decreased expression of the mediators necessary for viral entry into the respiratory epithelium and differences in the immune system responses in children. Specifically, decreased expression of proteins, including angiotensin-converting enzyme 2 (ACE2) and Transmembrane Serine Protease 2 (TMPRSS2) in the airway epithelium in children may prevent viral entry. The immune system differences may include a relative preponderance of CD4+ T cells, decreased neutrophil infiltration, decreased production of proinflammatory cytokines, and increased production of immunomodulatory cytokines in children compared with adults. Notably, the developing lung in children may have a greater capacity to recover and repair after viral infection. Understanding the relative contributions of the above processes to the protective phenotype in the developing lung can guide the trial of the appropriate therapies in adults.
Keywords: COVID-19; SARS-CoV-2; age-based susceptibility; children; coronavirus; pediatric lung.
Conflict of interest statement
No conflicts of interest, financial or otherwise, are declared by the authors.
Figures
References
-
- Castagnoli R, Votto M, Licari A, Brambilla I, Bruno R, Perlini S, Rovida F, Baldanti F, Marseglia GL. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection in children and adolescents: a systematic review. JAMA Pediatr. In press. doi: 10.1001/jamapediatrics.2020.1467. - DOI - PubMed
-
- Chen G, Wu D, Guo W, Cao Y, Huang D, Wang H, Wang T, Zhang X, Chen H, Yu H, Zhang X, Zhang M, Wu S, Song J, Chen T, Han M, Li S, Luo X, Zhao J, Ning Q. Clinical and immunological features of severe and moderate coronavirus disease 2019. J Clin Invest 130: 2620–2629, 2020. doi: 10.1172/JCI137244. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous