

Regional Disparities in Qualified Health Plans' Prior Authorization Requirements for HIV Pre-exposure Prophylaxis in the United States
- PMID: 32492164
- PMCID: PMC7272119
- DOI: 10.1001/jamanetworkopen.2020.7445
Regional Disparities in Qualified Health Plans' Prior Authorization Requirements for HIV Pre-exposure Prophylaxis in the United States
Abstract
Importance: With the goal of ending the HIV epidemic in the United States, access to HIV pre-exposure prophylaxis (PrEP) is essential to help curb new HIV infections. There has been differential uptake of PrEP by region, with the South lagging behind other regions. Discriminatory benefit design (benefit design that prevents or delays people with complex or expensive conditions from obtaining appropriate treatment) through prior authorization requirements could be a systemic barrier that contributes to the decreased PrEP uptake in the South.
Objectives: To investigate whether there are regional disparities in prior authorization requirements for combined tenofovir disoproxil fumarate and emtricitabine for qualified health plans (QHPs) and to assess whether any QHP characteristics explain the disparities.
Design, setting, and participants: This design was a cross-sectional study of QHPs offered in the 2019 Affordable Care Act Marketplace. The QHPs studied included all Affordable Care Act-compliant individual and small-group market plans in the United States.
Exposures: The primary exposure was the 4 census regions (Northeast, West, Midwest, and South). Additional covariates included other plan characteristics.
Main outcomes and measures: Prior authorization requirement for combined tenofovir disoproxil fumarate and emtricitabine at the QHP level.
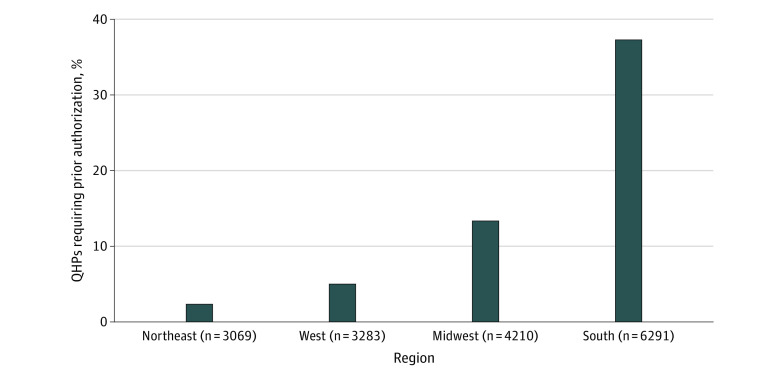
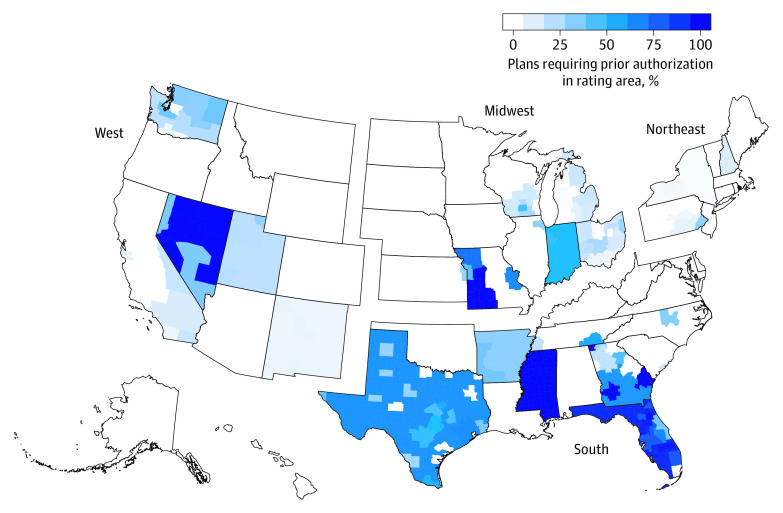
Results: In total, 16 853 QHPs were analyzed (18.2% in the Northeast, 19.5% in the West, 25.0% in the Midwest, and 37.3% in the South). Overall, 18.9% of QHPs required prior authorization for combined tenofovir disoproxil fumarate and emtricitabine. This percentage varied by region, with 2.3%, 6.2%, 13.3%, and 37.3% of plans requiring prior authorization in the Northeast, West, Midwest, and South, respectively. Compared with QHPs in the Northeast, QHPs in the South were 15.89 (95% CI, 12.57-20.09) times as likely to require prior authorization, whereas the Midwest and West were 5.69 (95% CI, 4.45-7.27) and 2.65 (95% CI, 2.02-3.47) times as likely, respectively. Other plan characteristics did not account for the regional variation.
Conclusions and relevance: Compared with QHPs in the Northeast, QHPs in the South were almost 16 times as likely to require prior authorization for PrEP, and the reasons for these disparities are unknown. The prior authorization requirement is a possible barrier to PrEP access in the South, which is the region of the United States with the most annual new HIV diagnoses. There is limited regulation of QHPs' prior authorization requirements. Federal- or state-level health policy laws may be necessary to remove this system-level barrier to ending the HIV epidemic in the United States.
Conflict of interest statement
Figures
References
-
- Farnham PG, Gopalappa C, Sansom SL, et al. . Updates of lifetime costs of care and quality-of-life estimates for HIV-infected persons in the United States: late versus early diagnosis and entry into care. J Acquir Immune Defic Syndr. 2013;64(2):183-189. doi:10.1097/QAI.0b013e3182973966 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
