

Variability in the Method of Gastrostomy Placement in Children
- PMID: 32492791
- PMCID: PMC7346129
- DOI: 10.3390/children7060053
Variability in the Method of Gastrostomy Placement in Children
Abstract
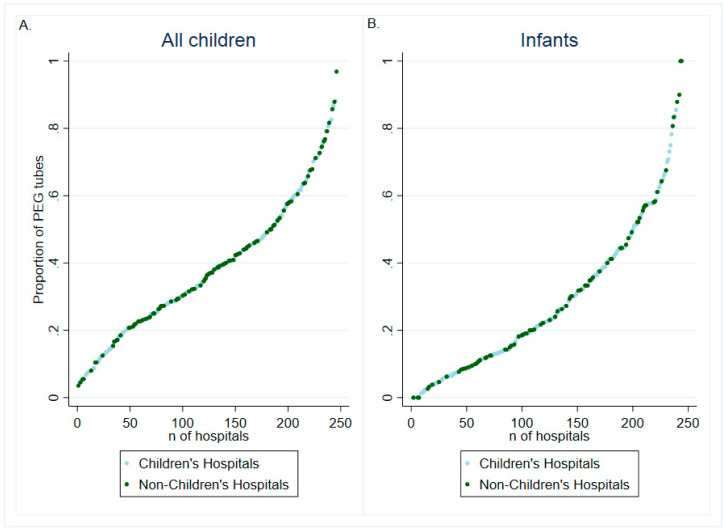
Although gastrostomy placement is one of the most common procedures performed in children, the optimal technique remains unclear. The purpose of this study was to evaluate variability in the method of gastrostomy tube placement in children in the United States. Patients <18 years old undergoing percutaneous endoscopic gastrostomy (PEG) or surgical gastrostomy (SG) (including open or laparoscopic) from 1997 to 2012 were identified using the Kids' Inpatient Database. Method of gastrostomy placement was evaluated using a multivariable mixed-effects logistic regression model with a random intercept term and a patient-age random-effect term. A total of 67,811 gastrostomy placements were performed during the study period. PEG was used in 36.6% of entries overall and was generally consistent over time. PEG placement was less commonly performed in infants (adjusted odds ratio [aOR] 0.30, 95%CI 0.26-0.33), children at urban hospitals (aOR: 0.38, 95%CI 0.18-0.82), and children cared for at children's hospitals (aOR 0.57, 95%CI 0.48-0.69) and was more commonly performed in children with private insurance (aOR 1.17, 95%CI 1.09-1.25). Dramatic variability in PEG use was identified between centers, ranging from 0% to 100%. The random intercept and slope terms significantly improved the model, confirming significant center-level variability and increased variability among patients <1 year old. These findings emphasize the need to further evaluate the safest method of gastrostomy placement in children, in particular among the youngest patients in whom practice varies the most.
Keywords: children; gastrostomy; technique; variability.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Sandberg F., Viktorsdottir M.B., Salo M., Stenstrom P., Arnbjornsson E. Comparison of major complications in children after laparoscopy-assisted gastrostomy and percutaneous endoscopic gastrostomy placement: A meta-analysis. Pediatr. Surg. Int. 2018;34:1321–1327. doi: 10.1007/s00383-018-4358-6. - DOI - PMC - PubMed
-
- Suksamanapun N., Mauritz F.A., Franken J., van der Zee D.C., van Herwaarden-Lindeboom M.Y. Laparoscopic versus percutaneous endoscopic gastrostomy placement in children: Results of a systematic review and meta-analysis. J. Minim. Access. Surg. 2017;13:81–88. doi: 10.4103/0972-9941.181776. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
