

Thoughts on the alveolar phase of COVID-19
- PMID: 32493030
- PMCID: PMC7347958
- DOI: 10.1152/ajplung.00126.2020
Thoughts on the alveolar phase of COVID-19
Abstract
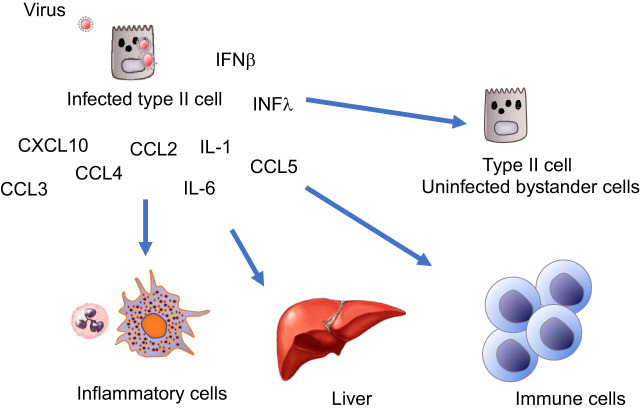
COVID-19 can be divided into three clinical stages, and one can speculate that these stages correlate with where the infection resides. For the asymptomatic phase, the infection mostly resides in the nose, where it elicits a minimal innate immune response. For the mildly symptomatic phase, the infection is mostly in the pseudostratified epithelium of the larger airways and is accompanied by a more vigorous innate immune response. In the conducting airways, the epithelium can recover from the infection, because the keratin 5 basal cells are spared and they are the progenitor cells for the bronchial epithelium. There may be more severe disease in the bronchioles, where the club cells are likely infected. The devastating third phase is in the gas exchange units of the lung, where ACE2-expressing alveolar type II cells and perhaps type I cells are infected. The loss of type II cells results in respiratory insufficiency due to the loss of pulmonary surfactant, alveolar flooding, and possible loss of normal repair, since type II cells are the progenitors of type I cells. The loss of type I and type II cells will also block normal active resorption of alveolar fluid. Subsequent endothelial damage leads to transudation of plasma proteins, formation of hyaline membranes, and an inflammatory exudate, characteristic of ARDS. Repair might be normal, but if the type II cells are severely damaged alternative pathways for epithelial repair may be activated, which would result in some residual lung disease.
Keywords: ACE2; SARS-CoV-2; type II cells.
Conflict of interest statement
No conflicts of interest, financial or otherwise, are declared by the author.
Figures


References
-
- Aevermann BD, Pickett BE, Kumar S, Klem EB, Agnihothram S, Askovich PS, Bankhead A 3rd, Bolles M, Carter V, Chang J, Clauss TR, Dash P, Diercks AH, Eisfeld AJ, Ellis A, Fan S, Ferris MT, Gralinski LE, Green RR, Gritsenko MA, Hatta M, Heegel RA, Jacobs JM, Jeng S, Josset L, Kaiser SM, Kelly S, Law GL, Li C, Li J, Long C, Luna ML, Matzke M, McDermott J, Menachery V, Metz TO, Mitchell H, Monroe ME, Navarro G, Neumann G, Podyminogin RL, Purvine SO, Rosenberger CM, Sanders CJ, Schepmoes AA, Shukla AK, Sims A, Sova P, Tam VC, Tchitchek N, Thomas PG, Tilton SC, Totura A, Wang J, Webb-Robertson BJ, Wen J, Weiss JM, Yang F, Yount B, Zhang Q, McWeeney S, Smith RD, Waters KM, Kawaoka Y, Baric R, Aderem A, Katze MG, Scheuermann RH. A comprehensive collection of systems biology data characterizing the host response to viral infection. Sci Data 1: 140033, 2014. doi: 10.1038/sdata.2014.33. - DOI - PMC - PubMed
-
- Chan JF, Zhang AJ, Yuan S, Poon VK, Chan CC, Lee AC, Chan WM, Fan Z, Tsoi HW, Wen L, Liang R, Cao J, Chen Y, Tang K, Luo C, Cai JP, Kok KH, Chu H, Chan KH, Sridhar S, Chen Z, Chen H, To KK, Yuen KY. Simulation of the clinical and pathological manifestations of Coronavirus Disease 2019 (COVID-19) in golden Syrian hamster model: implications for disease pathogenesis and transmissibility. Clin Infect Dis. In press. doi: 10.1093/cid/ciaa325. - DOI - PMC - PubMed
-
- Correll KA, Edeen KE, Zemans RL, Redente EF, Serban KA, Curran-Everett D, Edelman BL, Mikels-Vigdal A, Mason RJ. Transitional human alveolar type II epithelial cells suppress extracellular matrix and growth factor gene expression in lung fibroblasts. Am J Physiol Lung Cell Mol Physiol 317: L283–L294, 2019. doi: 10.1152/ajplung.00337.2018. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous