

The effect of intraoperative lidocaine infusion on opioid consumption and pain after totally extraperitoneal laparoscopic inguinal hernioplasty: a randomized controlled trial
- PMID: 32493276
- PMCID: PMC7268281
- DOI: 10.1186/s12871-020-01054-2
The effect of intraoperative lidocaine infusion on opioid consumption and pain after totally extraperitoneal laparoscopic inguinal hernioplasty: a randomized controlled trial
Abstract
Background: As a component of multimodal analgesia, the administration of systemic lidocaine is a well-known technique. We aimed to evaluate the efficacy of lidocaine infusion on postoperative pain-related outcomes in patients undergoing totally extraperitoneal (TEP) laparoscopies inguinal hernioplasty.
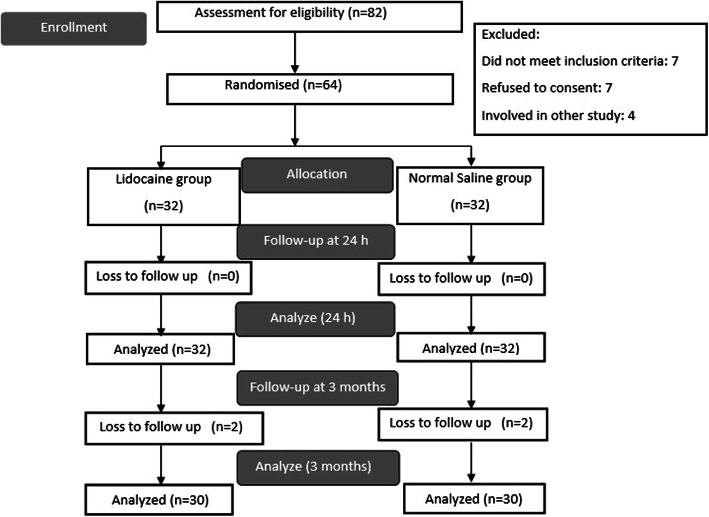
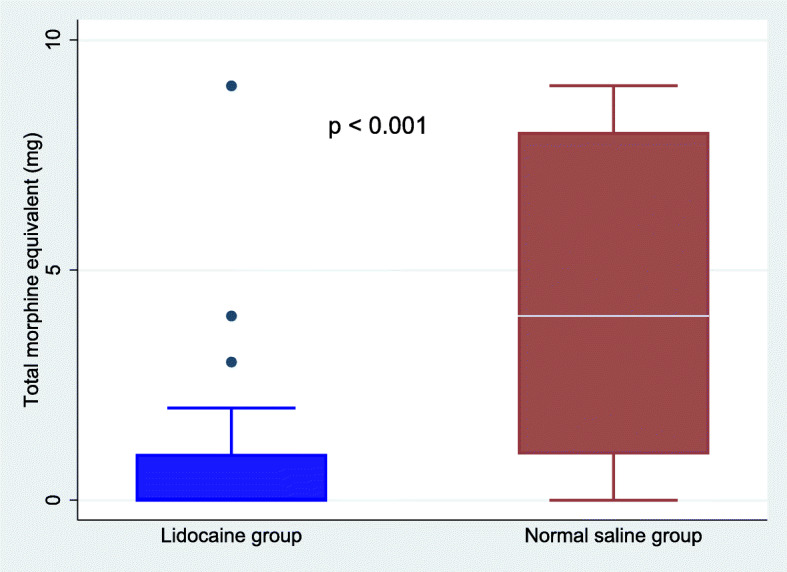
Methods: In this randomized controlled double-blind study, we recruited 64 patients to receive either lidocaine 2% (intravenous bolus 1.5 mg. kg - 1 followed by an infusion of 2 mg. kg- 1. h- 1), or an equal volume of normal saline. The infusion was initiated just before the induction of anesthesia and discontinued after tracheal extubation. The primary outcome of the study was postoperative morphine equivalent consumption up to 24 h after surgery. Secondary outcomes included postoperative pain scores, nausea/vomiting (PONV), sedation, quality of recovery (scores based on QoR-40 questionnaire), patient satisfaction, and the incidence of chronic pain.
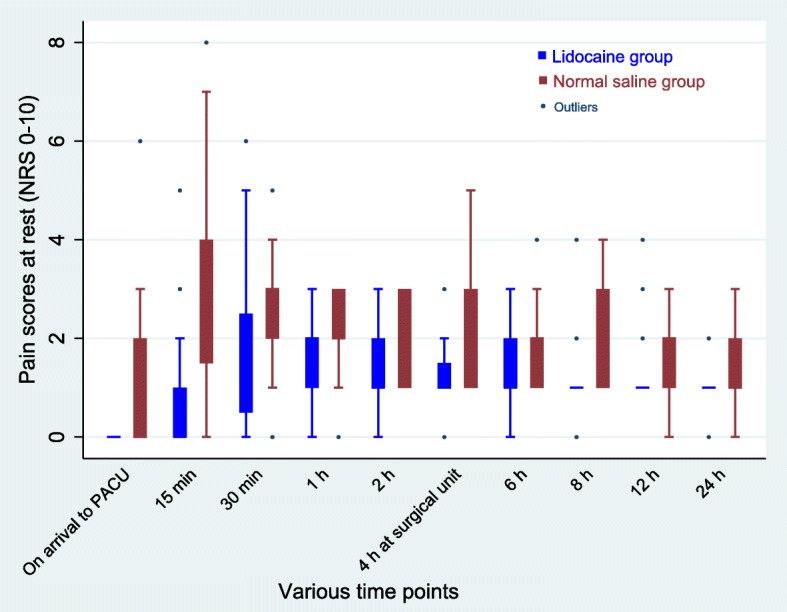
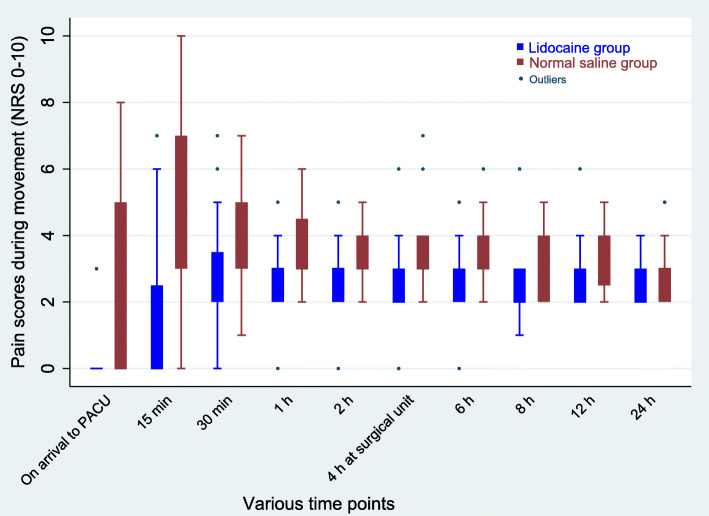
Results: The median (IQR) cumulative postoperative morphine equivalent consumption in the first 24 h was 0 (0-1) mg in the lidocaine group and 4 [1-8] mg in the saline group (p < 0.001). Postoperative pain intensity at rest and during movement at various time points in the first 24 h were significantly lower in the lidocaine group compared with the saline group (p < 0.05). Fewer patients reported PONV in the lidocaine group than in the saline group (p < 0.05). Median QoR scores at 24 h after surgery were significantly better in the lidocaine group (194 (194-196) than saline group 184 (183-186) (p < 0.001). Patients receiving lidocaine were more satisfied with postoperative analgesia than those receiving saline (p = 0.02). No difference was detected in terms of postoperative sedation and chronic pain after surgery.
Conclusions: Intraoperative lidocaine infusion for laparoscopic TEP inguinal hernioplasty reduces opioid consumption, pain intensity, PONV and improves the quality of recovery and patient satisfaction.
Trial registration: ClinicalTrials.gov- NCT02601651. Date of registration: November 10, 2015.
Keywords: Inguinal hernia; Laparoscopy; Lidocaine; Opioid analgesic; Postoperative pain.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
The effect of intraoperative lidocaine versus esmolol infusion on postoperative analgesia in laparoscopic cholecystectomy: a randomized clinical trial.BMC Anesthesiol. 2019 Nov 4;19(1):198. doi: 10.1186/s12871-019-0874-8. BMC Anesthesiol. 2019. PMID: 31684867 Free PMC article. Clinical Trial.
-
Effects of lidocaine, dexmedetomidine, and their combination infusion on postoperative nausea and vomiting following laparoscopic hysterectomy: a randomized controlled trial.BMC Anesthesiol. 2021 Aug 4;21(1):199. doi: 10.1186/s12871-021-01420-8. BMC Anesthesiol. 2021. PMID: 34348668 Free PMC article. Clinical Trial.
-
Opioid-free versus opioid-based anesthesia for day surgery laparoscopic inguinal hernia repair under ERAS protocol: a randomized non-inferiority trial.Hernia. 2025 Jul 9;29(1):225. doi: 10.1007/s10029-025-03410-y. Hernia. 2025. PMID: 40632161 Clinical Trial.
-
Perioperative intravenous lidocaine infusion improves postoperative analgesia after hysterectomy: a systematic review and meta-analysis of randomized controlled trials.Int J Surg. 2025 Jan 1;111(1):1265-1274. doi: 10.1097/JS9.0000000000001942. Int J Surg. 2025. PMID: 38976912 Free PMC article.
-
Efficacy of intraoperative intravenous lidocaine for postoperative analgesia following bariatric surgery: a meta-analysis of randomized controlled studies.Surg Obes Relat Dis. 2022 Jan;18(1):135-147. doi: 10.1016/j.soard.2021.08.014. Epub 2021 Sep 1. Surg Obes Relat Dis. 2022. PMID: 34565683 Review.
Cited by
-
Intravenous Infusion of Lidocaine Can Accelerate Postoperative Early Recovery in Patients Undergoing Surgery for Obstructive Sleep Apnea.Med Sci Monit. 2021 Feb 2;27:e926990. doi: 10.12659/MSM.926990. Med Sci Monit. 2021. PMID: 33529177 Free PMC article. Review.
-
Comparison of the effects of intravenous lignocaine and ketamine on postoperative pain after lower abdominal surgeries under general anaesthesia.Indian J Anaesth. 2023 Feb;67(Suppl 1):S41-S47. doi: 10.4103/ija.ija_691_22. Epub 2023 Feb 10. Indian J Anaesth. 2023. PMID: 37065953 Free PMC article.
-
Effect of intravenous lignocaine infusion on propofol requirement using a closed-loop anaesthesia delivery system: A randomised controlled study.Indian J Anaesth. 2025 Jun;69(6):587-593. doi: 10.4103/ija.ija_830_24. Epub 2025 May 14. Indian J Anaesth. 2025. PMID: 40470388 Free PMC article.
-
Intravenous Lidocaine for Postoperative Analgesia in 90 patients After Total Knee Arthroplasty and Limb Fractures.Med Sci Monit. 2022 Mar 23;28:e935852. doi: 10.12659/MSM.935852. Med Sci Monit. 2022. PMID: 35320161 Free PMC article.
-
Opioid-Sparing Analgesia Impacts the Perioperative Anesthetic Management in Major Abdominal Surgery.Medicina (Kaunas). 2022 Mar 28;58(4):487. doi: 10.3390/medicina58040487. Medicina (Kaunas). 2022. PMID: 35454326 Free PMC article. Clinical Trial.
References
-
- Gan TJ, Joshi GP, Zhao SZ, Hanna DB, Cheung RY, Chen C. Presurgical intravenous parecoxib sodium and follow-up oral valdecoxib for pain management after laparoscopic cholecystectomy surgery reduces opioid requirements and opioid-related adverse effects. Acta Anaesthesiol Scand. 2004;48:1194–1207. doi: 10.1111/j.1399-6576.2004.00495.x. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
