

Reach out behavioral intervention for hypertension initiated in the emergency department connecting multiple health systems: study protocol for a randomized control trial
- PMID: 32493502
- PMCID: PMC7268693
- DOI: 10.1186/s13063-020-04340-z
Reach out behavioral intervention for hypertension initiated in the emergency department connecting multiple health systems: study protocol for a randomized control trial
Abstract
Background: Hypertension is the most important modifiable risk factor for cardiovascular disease, the leading cause of mortality in the United States. The Emergency Department represents an underutilized opportunity to impact difficult-to-reach populations. There are 136 million visits to the Emergency Department each year and nearly all have at least one blood pressure measured and recorded. Additionally, an increasing number of African Americans and socioeconomically disadvantaged patients are overrepresented in the Emergency Department patient population. In the age of electronic health records and mobile health, the Emergency Department has the potential to become an integral partner in chronic disease management. The electronic health records in conjunction with mobile health behavior interventions can be leveraged to identify hypertensive patients to impact otherwise unreached populations.
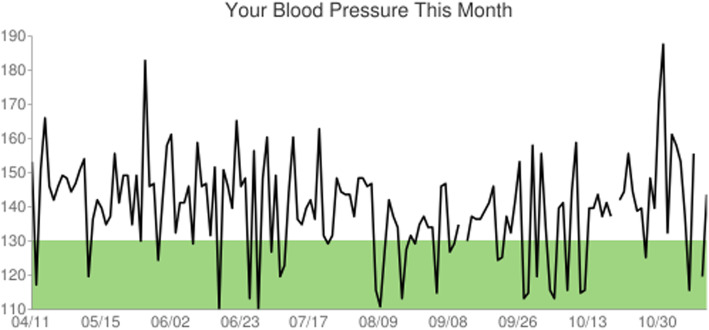
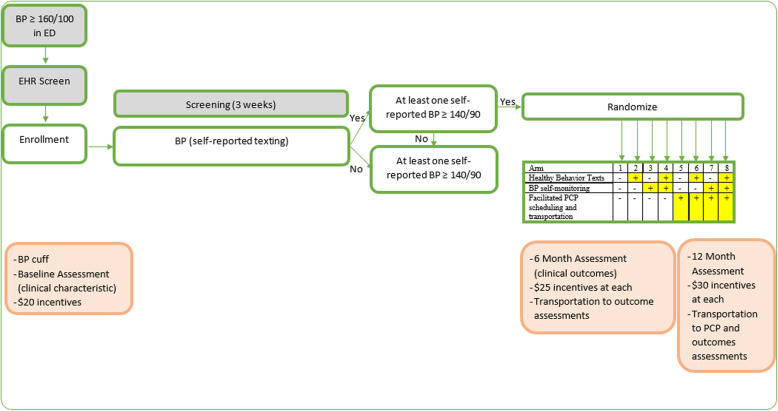
Methods: Reach Out is a factorial trial studying multicomponent, behavioral interventions to reduce blood pressure in the Emergency Department patient population. Potential participants are identified by automated alerts from the electronic health record and, following consent, receive a blood pressure cuff to take home. During the initial screening phase, they are prompted to submit weekly blood pressure readings. Responders with persistent hypertension are then randomized into one of three component arms, consisting of varying intensity levels: (1) healthy behavior text messaging (daily vs. none), (2) blood pressure self-monitoring (daily vs. weekly), and (3) facilitated primary care provider appointment scheduling and transportation (yes vs. no). If participants are randomized to receive facilitated primary care provider appointment scheduling and are not established with a primary care provider, care will be established at a local Federally Qualified Health Center. Participants are followed for 12 months.
Discussion: The Reach Out study is designed to determine which behavioral intervention components or 'dose' of components contributes to a reduction in systolic blood pressure after 1 year (Aim 1). The study will also assess the effect of primary care provider appointment assistance on total primary care follow-up visits of hypertensive patients treated in an urban, safety net Emergency Department (Aim 2). Ideally, the Reach Out system will contribute to hypertension management, serving as a model for safety net hospitals and Federally Qualified Health Centers to improve chronic disease management in underserved communities.
Trial registration: This study was registered at clinicaltrials.gov, identifier NCT03422718. The record was first available to the public on January 30, 2018 prior to the enrollment of patients on March 25, 2019.
Keywords: Emergency medicine; Hypertension; Multiphase optimization strategy; Randomized clinical trial; Randomized controlled trial.
Conflict of interest statement
WJM, MD, KMK, AF, EC, JC, DB, SM, RC, LRB, DB, LS, CW, and DT report no financial or other competing interests.
Figures


References
-
- Burke LE, Ma J, Azar KM, Bennett GG, Peterson ED, Zheng Y, et al. Current science on consumer use of mobile health for cardiovascular disease prevention: a scientific statement from the american heart association. Circulation. 2015;132(12):1157–1213. doi: 10.1161/CIR.0000000000000232. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
