

Performance of a guideline-recommended algorithm for prognostication of poor neurological outcome after cardiac arrest
- PMID: 32494928
- PMCID: PMC7527324
- DOI: 10.1007/s00134-020-06080-9
Performance of a guideline-recommended algorithm for prognostication of poor neurological outcome after cardiac arrest
Abstract
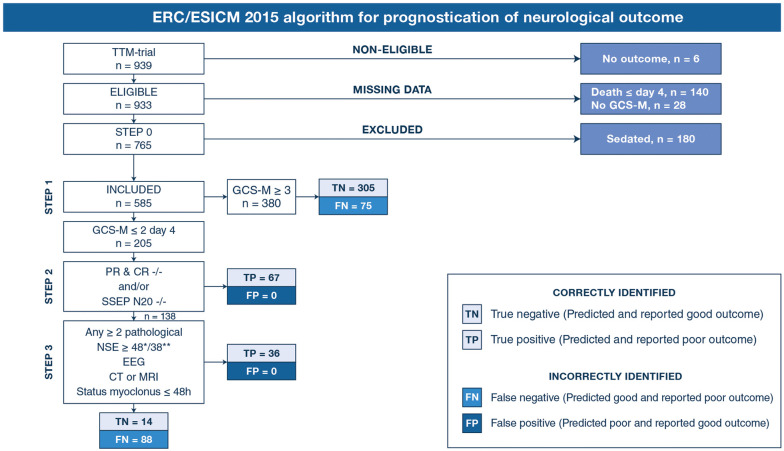
Purpose: To assess the performance of a 4-step algorithm for neurological prognostication after cardiac arrest recommended by the European Resuscitation Council (ERC) and the European Society of Intensive Care Medicine (ESICM).
Methods: Retrospective descriptive analysis with data from the Target Temperature Management (TTM) Trial. Associations between predicted and actual neurological outcome were investigated for each step of the algorithm with results from clinical neurological examinations, neuroradiology (CT or MRI), neurophysiology (EEG and SSEP) and serum neuron-specific enolase. Patients examined with Glasgow Coma Scale Motor Score (GCS-M) on day 4 (72-96 h) post-arrest and available 6-month outcome were included. Poor outcome was defined as Cerebral Performance Category 3-5. Variations of the ERC/ESICM algorithm were explored within the same cohort.
Results: The ERC/ESICM algorithm identified poor outcome patients with 38.7% sensitivity (95% CI 33.1-44.7) and 100% specificity (95% CI 98.8-100) in a cohort of 585 patients. An alternative cut-off for serum neuron-specific enolase, an alternative EEG-classification and variations of the GCS-M had minor effects on the sensitivity without causing false positive predictions. The highest overall sensitivity, 42.5% (95% CI 36.7-48.5), was achieved when prognosticating patients irrespective of GCS-M score, with 100% specificity (95% CI 98.8-100) remaining.
Conclusion: The ERC/ESICM algorithm and all exploratory multimodal variations thereof investigated in this study predicted poor outcome without false positive predictions and with sensitivities 34.6-42.5%. Our results should be validated prospectively, preferably in patients where withdrawal of life-sustaining therapy is uncommon to exclude any confounding from self-fulfilling prophecies.
Keywords: Cardiac arrest; Coma; Guideline algorithm; Prognostic accuracy; Prognostication.
Conflict of interest statement
MMK, EW, SB, NM, ID, AL, PS, GL, JH, JK, CR, CH, SU and NN report no conflicts of interests. TC and HF participated in the 2014 ERC/ESICM advisory statement on neuroprognostication after cardiac arrest.
Figures


Comment in
-
ERC-ESICM guidelines for prognostication after cardiac arrest: time for an update.Intensive Care Med. 2020 Oct;46(10):1901-1903. doi: 10.1007/s00134-020-06224-x. Epub 2020 Sep 4. Intensive Care Med. 2020. PMID: 32886207 No abstract available.
References
-
- Sandroni C, Cariou A, Cavallaro F, Cronberg T, Friberg H, Hoedemaekers C, Horn J, Nolan JP, Rossetti AO, Soar J. Prognostication in comatose survivors of cardiac arrest: an advisory statement from the European Resuscitation Council and the European Society of Intensive Care Medicine. Resuscitation. 2014;85(12):1779–1789. doi: 10.1016/j.resuscitation.2014.08.011. - DOI - PubMed
-
- Westhall E, Rossetti AO, van Rootselaar AF, Wesenberg Kjaer T, Horn J, Ullen S, Friberg H, Nielsen N, Rosen I, Aneman A, Erlinge D, Gasche Y, Hassager C, Hovdenes J, Kjaergaard J, Kuiper M, Pellis T, Stammet P, Wanscher M, Wetterslev J, Wise MP, Cronberg T, Investigators TT-t Standardized EEG interpretation accurately predicts prognosis after cardiac arrest. Neurology. 2016;86(16):1482–1490. doi: 10.1212/wnl.0000000000002462. - DOI - PMC - PubMed
-
- Backman S, Cronberg T, Friberg H, Ullén S, Horn J, Kjaergaard J, Hassager C, Wanscher M, Nielsen N, Westhall E. Highly malignant routine EEG predicts poor prognosis after cardiac arrest in the Target Temperature Management trial. Resuscitation. 2018;131:24–28. doi: 10.1016/j.resuscitation.2018.07.024. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
