

A case of unplanned pregnancy at 2 months after uterine curettage in a patient with a hydatidiform mole
- PMID: 32495669
- PMCID: PMC7273807
- DOI: 10.1177/0300060520925961
A case of unplanned pregnancy at 2 months after uterine curettage in a patient with a hydatidiform mole
Abstract
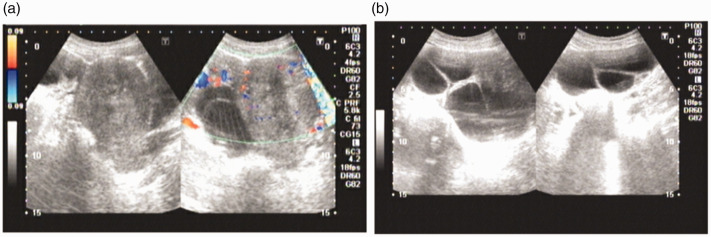
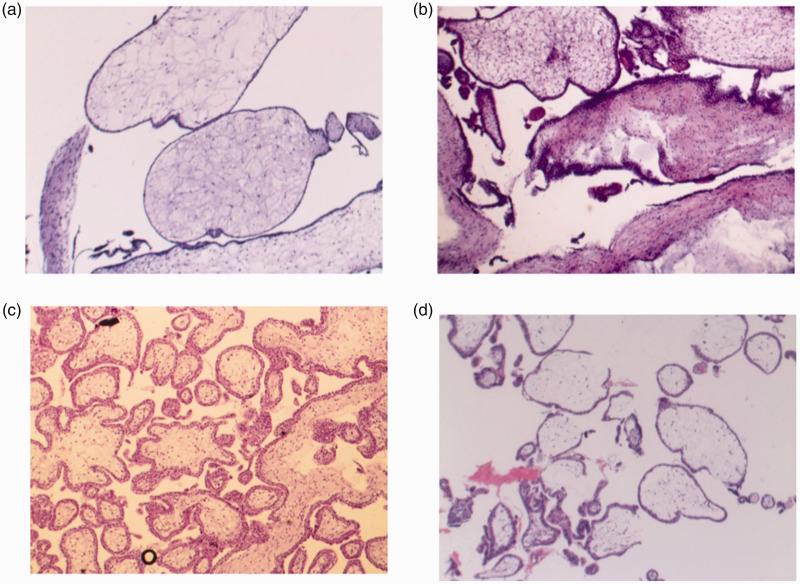
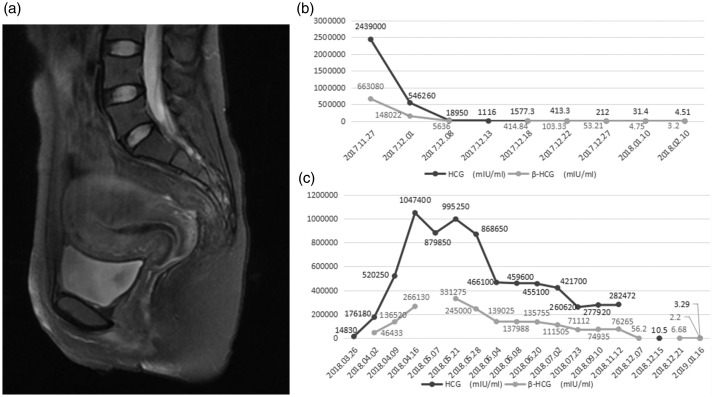
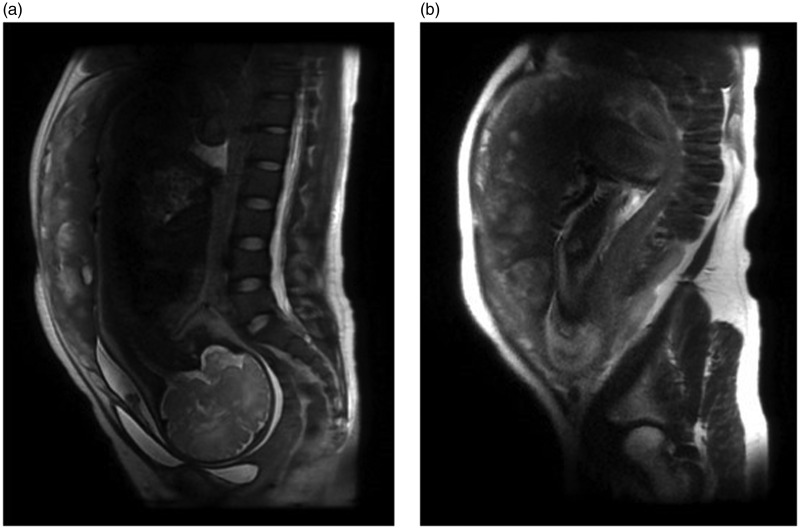
Whether an unplanned pregnancy should be terminated during follow-up of a hydatidiform mole is controversial. We report a patient who had an unplanned pregnancy with a hydatidiform mole at 2 months after uterine curettage when the human chorionic gonadotropin level had decreased to a negative value. Hydatidiform mole was confirmed by histopathology. Uterine curettage was performed twice and regular follow-ups were performed after surgery. The patient achieved a full-term pregnancy. The Apgar score of the newborn was 10 at 1, 5, and 10 minutes, and the newborn had no malformations. We conclude that the pregnancy outcome might be good in an unplanned pregnancy when the human chorionic gonadotropin level is negative.
Keywords: B-ultrasonography; Hydatidiform mole; human chorionic gonadotropin; pregnancy; trophoblastic neoplasm; uterine curettage.
Figures
Similar articles
-
Giant complete hydatidiform mole: a case report and review of the literature.J Med Case Rep. 2024 Jun 13;18(1):277. doi: 10.1186/s13256-024-04474-7. J Med Case Rep. 2024. PMID: 38867300 Free PMC article. Review.
-
Heterotopic pregnancy: a case report of intrauterine hydatidiform mole with tubal pregnancy.J Int Med Res. 2024 Jun;52(6):3000605241258572. doi: 10.1177/03000605241258572. J Int Med Res. 2024. PMID: 38869107 Free PMC article.
-
[Clinical characteristics and diagnosis of early hydatidiform mole].Zhonghua Fu Chan Ke Za Zhi. 2019 Nov 25;54(11):756-762. doi: 10.3760/cma.j.issn.0529-567x.2019.11.008. Zhonghua Fu Chan Ke Za Zhi. 2019. PMID: 31752459 Chinese.
-
The value of endometrial curettage in the follow-up of hydatidiform mole.Acta Obstet Gynecol Scand. 1988;67(7):649-51. doi: 10.3109/00016348809004280. Acta Obstet Gynecol Scand. 1988. PMID: 3247837
-
Partial hydatidiform mole with subsequent trophoblastic tumor; a case report.Eur J Obstet Gynecol Reprod Biol. 1991 Jun 5;40(1):73-7. doi: 10.1016/0028-2243(91)90048-p. Eur J Obstet Gynecol Reprod Biol. 1991. PMID: 1649776 Review.
Cited by
-
Complete hydatidiform mole in a 52-year-old postmenopausal woman: A case report and literature review.Case Rep Womens Health. 2021 Jun 19;31:e00338. doi: 10.1016/j.crwh.2021.e00338. eCollection 2021 Jul. Case Rep Womens Health. 2021. PMID: 34258236 Free PMC article.
References
-
- Hui P, Buza N, Murphy KM, et al. Hydatidiform moles: genetic basis and precision diagnosis. Annu Rev Pathol 2017; 12: 449–485. - PubMed
-
- Shaaban AM, Rezvani M, Haroun RR, et al. Gestational trophoblastic disease: clinical and imaging features. Radiographics 2017; 37: 681–700. - PubMed
-
- Xiang Y, Zhou Q, Wu XH, et al. Guidelines for diagnosis and treatment of gestational trophoblastic diseases (4th edition). Chinese J Pract Gynecol Obstet 2018; 34: 994–1001.
-
- Ngan HY, Seckl MJ, Berkowitz RS, et al. Update on the diagnosis and management of gestational trophoblastic disease. Int J Gynecol Obstet 2018; 143: 79–85. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
