

Sepsis With Preexisting Heart Failure: Management of Confounding Clinical Features
- PMID: 32495686
- PMCID: PMC7970342
- DOI: 10.1177/0885066620928299
Sepsis With Preexisting Heart Failure: Management of Confounding Clinical Features
Abstract
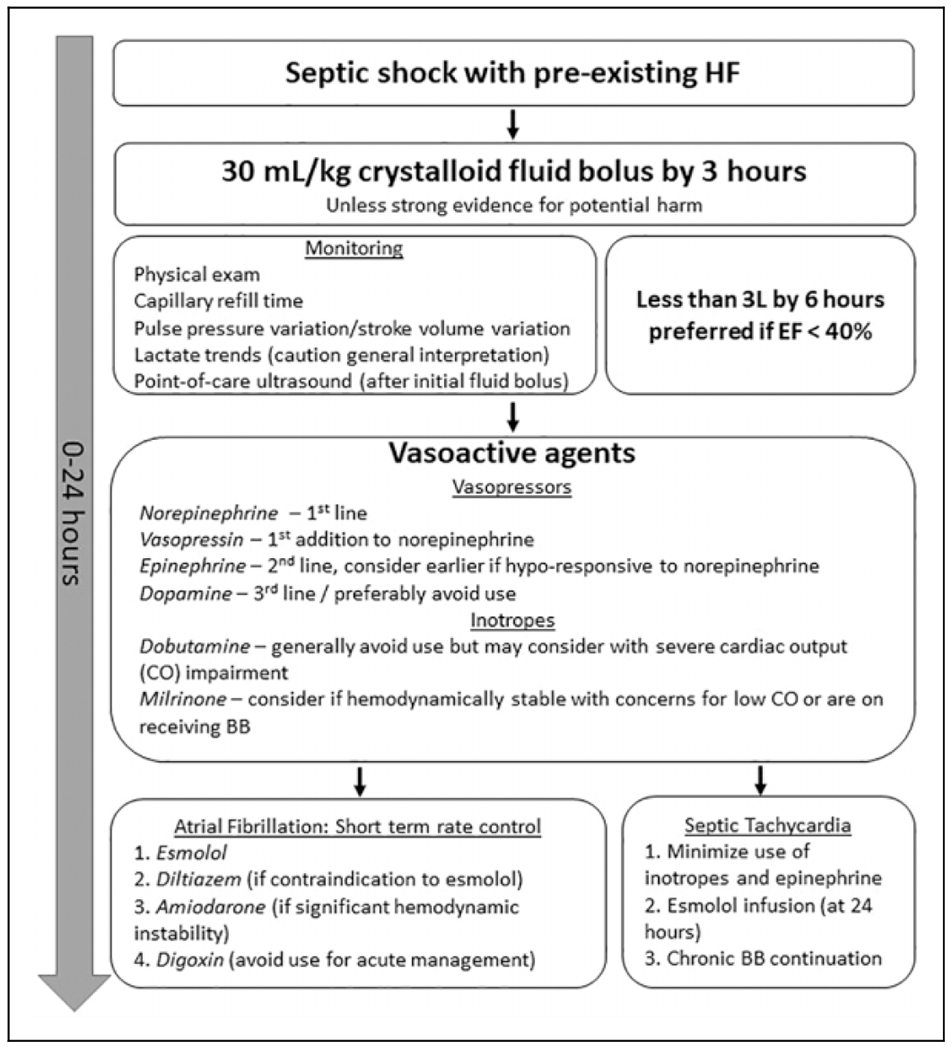
Preexisting heart failure (HF) in patients with sepsis is associated with worse clinical outcomes. Core sepsis management includes aggressive volume resuscitation followed by vasopressors (and potentially inotropes) if fluid is inadequate to restore perfusion; however, large fluid boluses and vasoactive agents are concerning amid the cardiac dysfunction of HF. This review summarizes evidence regarding the influence of HF on sepsis clinical outcomes, pathophysiologic concerns, resuscitation targets, hemodynamic interventions, and adjunct management (ie, antiarrhythmics, positive pressure ventilatory support, and renal replacement therapy) in patients with sepsis and preexisting HF. Patients with sepsis and preexisting HF receive less fluid during resuscitation; however, evidence suggests traditional fluid resuscitation targets do not increase the risk of adverse events in HF patients with sepsis and likely improve outcomes. Norepinephrine remains the most well-supported vasopressor for patients with sepsis with preexisting HF, while dopamine may induce more cardiac adverse events. Dobutamine should be used cautiously given its generally detrimental effects but may have an application when combined with norepinephrine in patients with low cardiac output. Management of chronic HF medications warrants careful consideration for continuation or discontinuation upon development of sepsis, and β-blockers may be appropriate to continue in the absence of acute hemodynamic decompensation. Optimal management of atrial fibrillation may include β-blockers after acute hemodynamic stabilization as they have also shown independent benefits in sepsis. Positive pressure ventilatory support and renal replacement must be carefully monitored for effects on cardiac function when HF is present.
Keywords: antiarrhythmics; fluids; heart failure; inotropes; resuscitation; sepsis; septic shock; vasopressors.
Conflict of interest statement
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Bloom MW, Greenberg B, Jaarsma T, et al. Heart failure with reduced ejection fraction. Nat Rev Dis Primers. 2017;3:17058. - PubMed
-
- Fleischmann C, Scherag A, Adhikari NK, et al. Assessment of global incidence and mortality of hospital-treated sepsis. Current estimates and limitations. Am J Respir Crit Care Med. 2016; 193(3):259–272. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
