

Early Experience With COVID-19 and Solid Organ Transplantation at a US High-volume Transplant Center
- PMID: 32496357
- PMCID: PMC7302089
- DOI: 10.1097/TP.0000000000003339
Early Experience With COVID-19 and Solid Organ Transplantation at a US High-volume Transplant Center
Abstract
Background: The novel coronavirus severe acute respiratory syndrome coronavirus 2 [coronavirus disease 2019 (COVID-19)] poses unique challenges for immunosuppressed patients. Solid organ transplant (SOT) recipients comprise a large proportion of this group, yet there is limited knowledge about the presentation, clinical course, and immunosuppression management of this novel infection among heart, lung, liver, pancreas, and kidney transplant recipients.
Methods: We present 21 SOT recipients diagnosed with COVID-19 between January 1, 2020 and April 22, 2020 at a US high-volume transplant center. Diagnostic workup, clinical course, immunosuppression/antiviral management, and immediate outcomes are described.
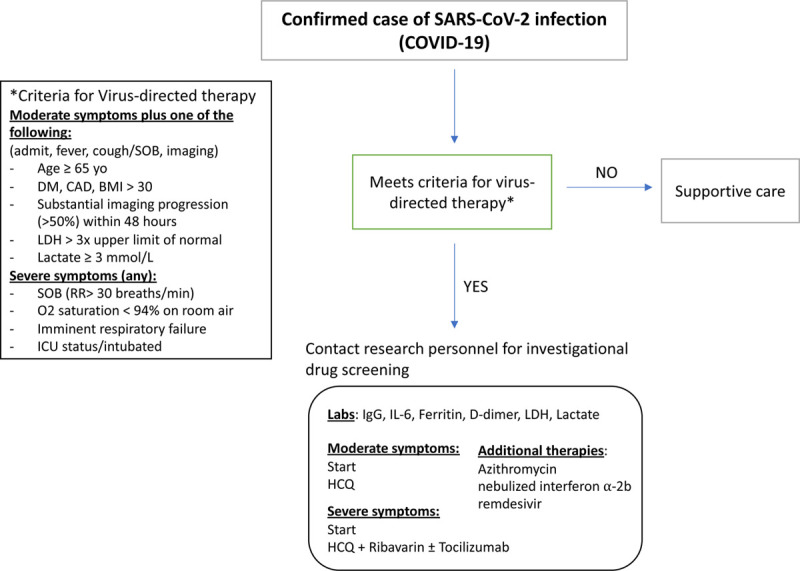
Results: Twenty-one (15.9%) of 132 symptomatic patients tested were positive. Mean age at diagnosis was 54.8 ± 10.9 y. Median time from transplant was 5.58 y (interquartile range 2.25, 7.33). Median follow-up was 18 d (interquartile range 13, 30). Fourteen patients required inpatient management, with 7 (50%) placed in the intensive care unit (ICU). All transplant types were represented. Nearly 43% exhibited GI symptoms. Over half (56.2%) presented with elevated serum creatinine suggestive of acute kidney injury. The majority of patients (5/7) with concomitant infections at baseline required the ICU. Eighty percent received hydroxychloroquine ± azithromycin. Ten received toclizumab and/or ribavirin; 1 received remdesivir. Antimetabolites ± calcineurin inhibitors were held or reduced. Over half of hospitalized patients (8/14) were discharged home. Only 1 mortality (4.8%) to date, in a critically ill heart/kidney patient who had been in the ICU before diagnosis.
Conclusions: COVID-19 positive SOT at our institution had favorable short-term outcomes. Those with concomitant infections had more severe illness. More data will be available to evaluate long-term outcomes and disease impact on graft function.
Conflict of interest statement
The authors declare no funding or conflicts of interest.
Figures
References
-
- World Health Organization. Coronavirus disease 2019 (COVID-19): situation report, 72. 2020; 72
-
- Gainer SM, Patel SJ, Seethamraju H, et al. Increased mortality of solid organ transplant recipients with H1N1 infection: a single center experience. Clin Transplant. 2012; 26:229–237. doi:10.1111/j.1399-0012.2011.01443.x - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
