

Association of Noninvasive Oxygenation Strategies With All-Cause Mortality in Adults With Acute Hypoxemic Respiratory Failure: A Systematic Review and Meta-analysis
- PMID: 32496521
- PMCID: PMC7273316
- DOI: 10.1001/jama.2020.9524
Association of Noninvasive Oxygenation Strategies With All-Cause Mortality in Adults With Acute Hypoxemic Respiratory Failure: A Systematic Review and Meta-analysis
Abstract
Importance: Treatment with noninvasive oxygenation strategies such as noninvasive ventilation and high-flow nasal oxygen may be more effective than standard oxygen therapy alone in patients with acute hypoxemic respiratory failure.
Objective: To compare the association of noninvasive oxygenation strategies with mortality and endotracheal intubation in adults with acute hypoxemic respiratory failure.
Data sources: The following bibliographic databases were searched from inception until April 2020: MEDLINE, Embase, PubMed, Cochrane Central Register of Controlled Trials, CINAHL, Web of Science, and LILACS. No limits were applied to language, publication year, sex, or race.
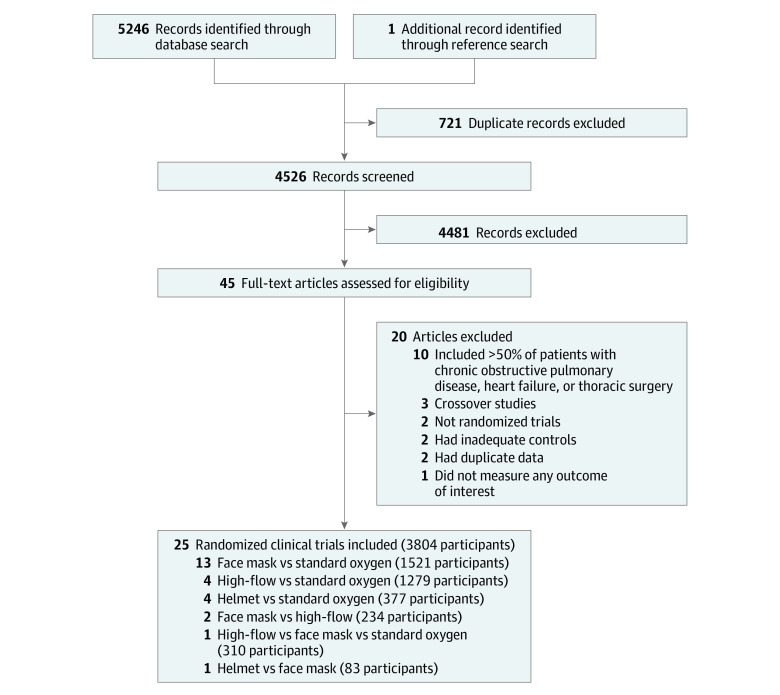
Study selection: Randomized clinical trials enrolling adult participants with acute hypoxemic respiratory failure comparing high-flow nasal oxygen, face mask noninvasive ventilation, helmet noninvasive ventilation, or standard oxygen therapy.
Data extraction and synthesis: Two reviewers independently extracted individual study data and evaluated studies for risk of bias using the Cochrane Risk of Bias tool. Network meta-analyses using a bayesian framework to derive risk ratios (RRs) and risk differences along with 95% credible intervals (CrIs) were conducted. GRADE methodology was used to rate the certainty in findings.
Main outcomes and measures: The primary outcome was all-cause mortality up to 90 days. A secondary outcome was endotracheal intubation up to 30 days.
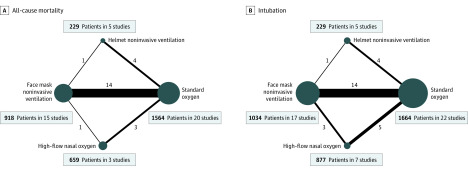
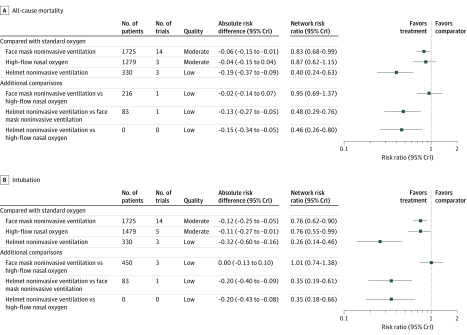
Results: Twenty-five randomized clinical trials (3804 participants) were included. Compared with standard oxygen, treatment with helmet noninvasive ventilation (RR, 0.40 [95% CrI, 0.24-0.63]; absolute risk difference, -0.19 [95% CrI, -0.37 to -0.09]; low certainty) and face mask noninvasive ventilation (RR, 0.83 [95% CrI, 0.68-0.99]; absolute risk difference, -0.06 [95% CrI, -0.15 to -0.01]; moderate certainty) were associated with a lower risk of mortality (21 studies [3370 patients]). Helmet noninvasive ventilation (RR, 0.26 [95% CrI, 0.14-0.46]; absolute risk difference, -0.32 [95% CrI, -0.60 to -0.16]; low certainty), face mask noninvasive ventilation (RR, 0.76 [95% CrI, 0.62-0.90]; absolute risk difference, -0.12 [95% CrI, -0.25 to -0.05]; moderate certainty) and high-flow nasal oxygen (RR, 0.76 [95% CrI, 0.55-0.99]; absolute risk difference, -0.11 [95% CrI, -0.27 to -0.01]; moderate certainty) were associated with lower risk of endotracheal intubation (25 studies [3804 patients]). The risk of bias due to lack of blinding for intubation was deemed high.
Conclusions and relevance: In this network meta-analysis of trials of adult patients with acute hypoxemic respiratory failure, treatment with noninvasive oxygenation strategies compared with standard oxygen therapy was associated with lower risk of death. Further research is needed to better understand the relative benefits of each strategy.
Conflict of interest statement
Figures
Comment in
-
Alternatives to Invasive Ventilation in the COVID-19 Pandemic.JAMA. 2020 Jul 7;324(1):43-44. doi: 10.1001/jama.2020.9611. JAMA. 2020. PMID: 32496506 No abstract available.
-
Noninvasive Oxygenation Strategies for Acute Hypoxemic Respiratory Failure.JAMA. 2020 Nov 10;324(18):1905-1906. doi: 10.1001/jama.2020.18591. JAMA. 2020. PMID: 33170233 No abstract available.
