

Impact of Intrathecal Triple Therapy Versus Intrathecal Methotrexate on Disease-Free Survival for High-Risk B-Lymphoblastic Leukemia: Children's Oncology Group Study AALL1131
- PMID: 32496902
- PMCID: PMC7402996
- DOI: 10.1200/JCO.19.02892
Impact of Intrathecal Triple Therapy Versus Intrathecal Methotrexate on Disease-Free Survival for High-Risk B-Lymphoblastic Leukemia: Children's Oncology Group Study AALL1131
Abstract
Purpose: The high-risk stratum of Children's Oncology Group Study AALL1131 was designed to test the hypothesis that postinduction CNS prophylaxis with intrathecal triple therapy (ITT) including methotrexate, hydrocortisone, and cytarabine would improve the postinduction 5-year disease-free survival (DFS) compared with intrathecal methotrexate (IT MTX), when given on a modified augmented Berlin-Frankfurt-Münster backbone.
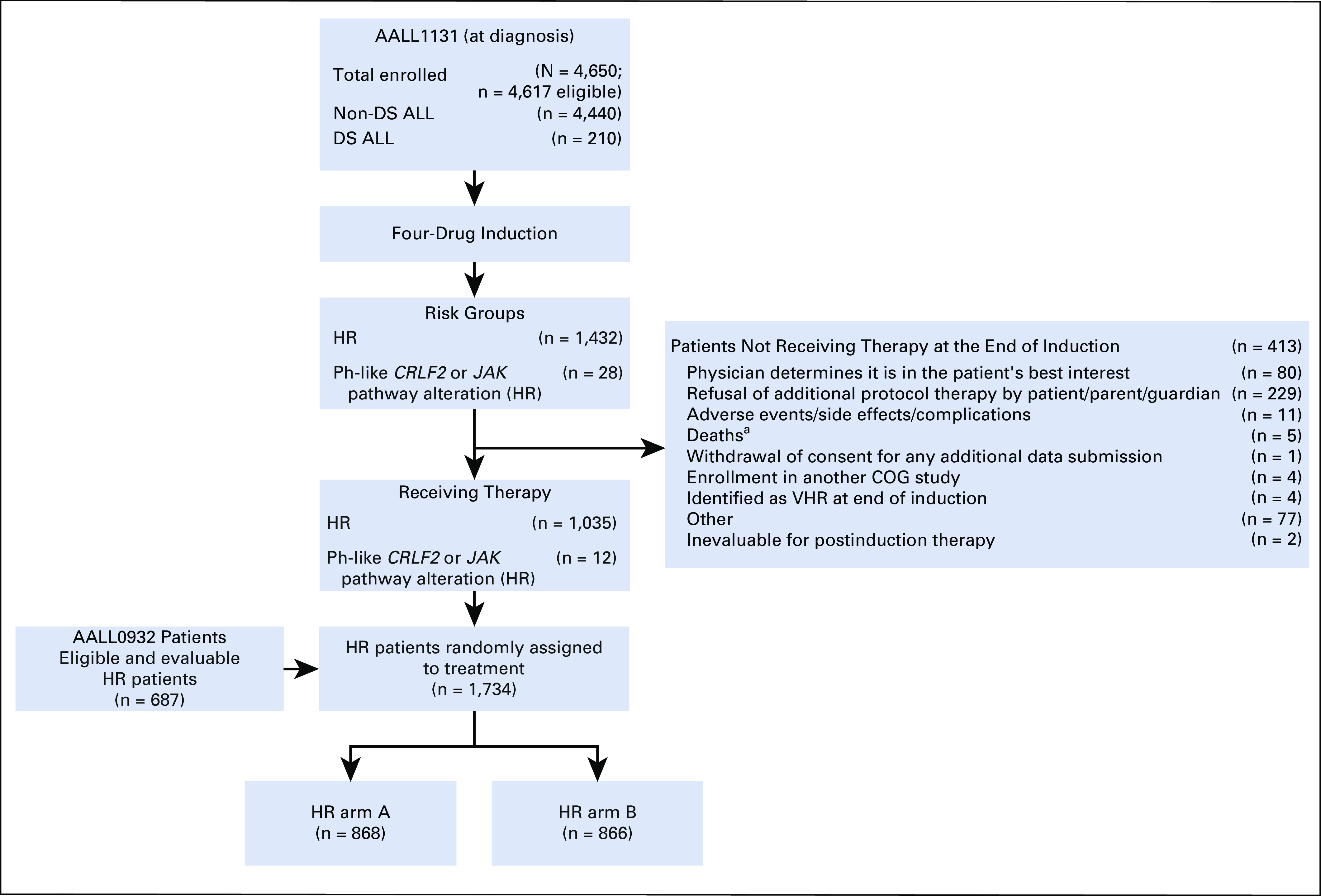
Patients and methods: Children with newly diagnosed National Cancer Institute (NCI) high-risk B-cell acute lymphoblastic leukemia (HR B-ALL) or NCI standard-risk B-ALL with defined minimal residual disease thresholds during induction were randomly assigned to receive postinduction IT MTX or ITT. Patients with CNS3-status disease were not eligible. Postinduction IT therapy was given for a total of 21 to 26 doses. Neurocognitive assessments were performed during therapy and during 1 year off therapy.
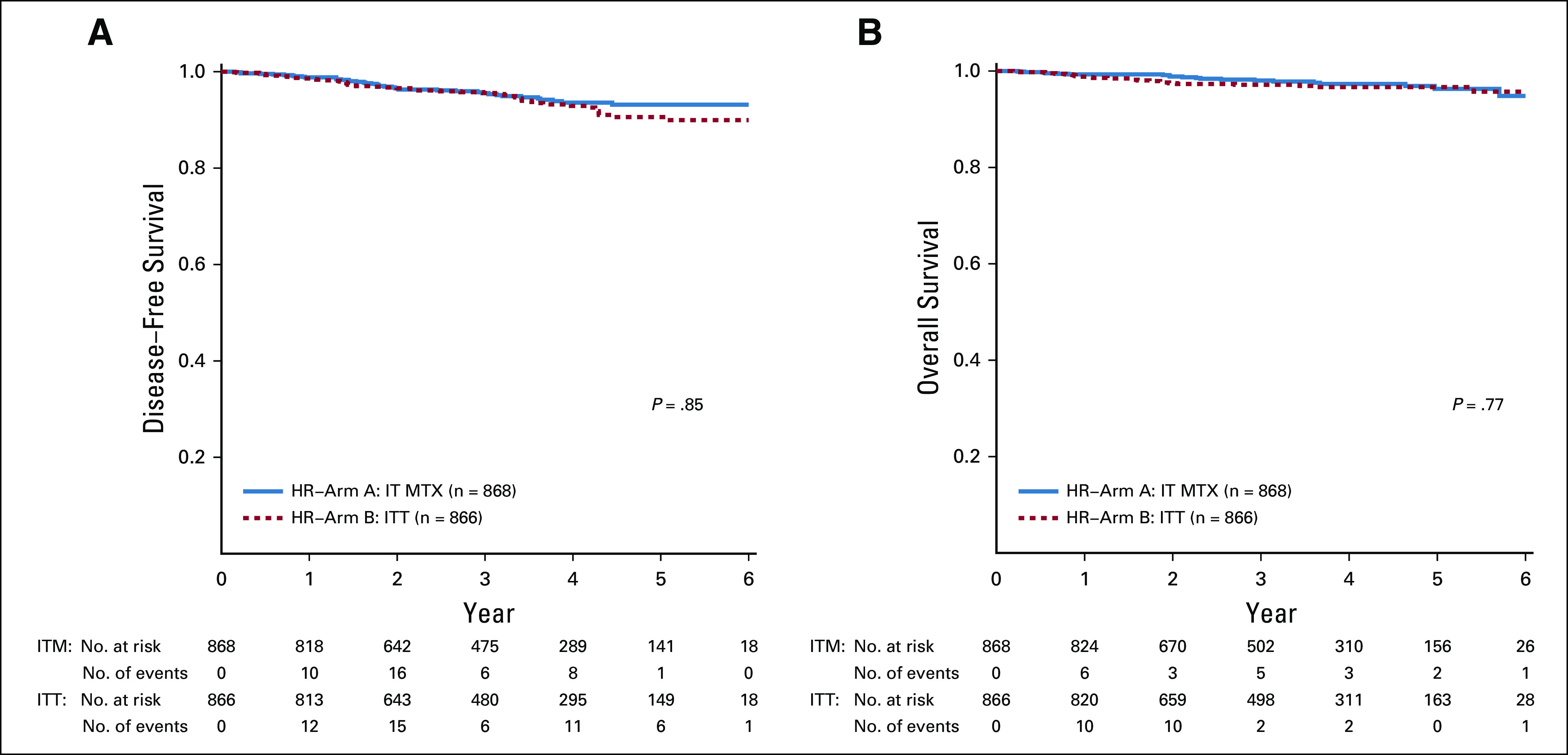
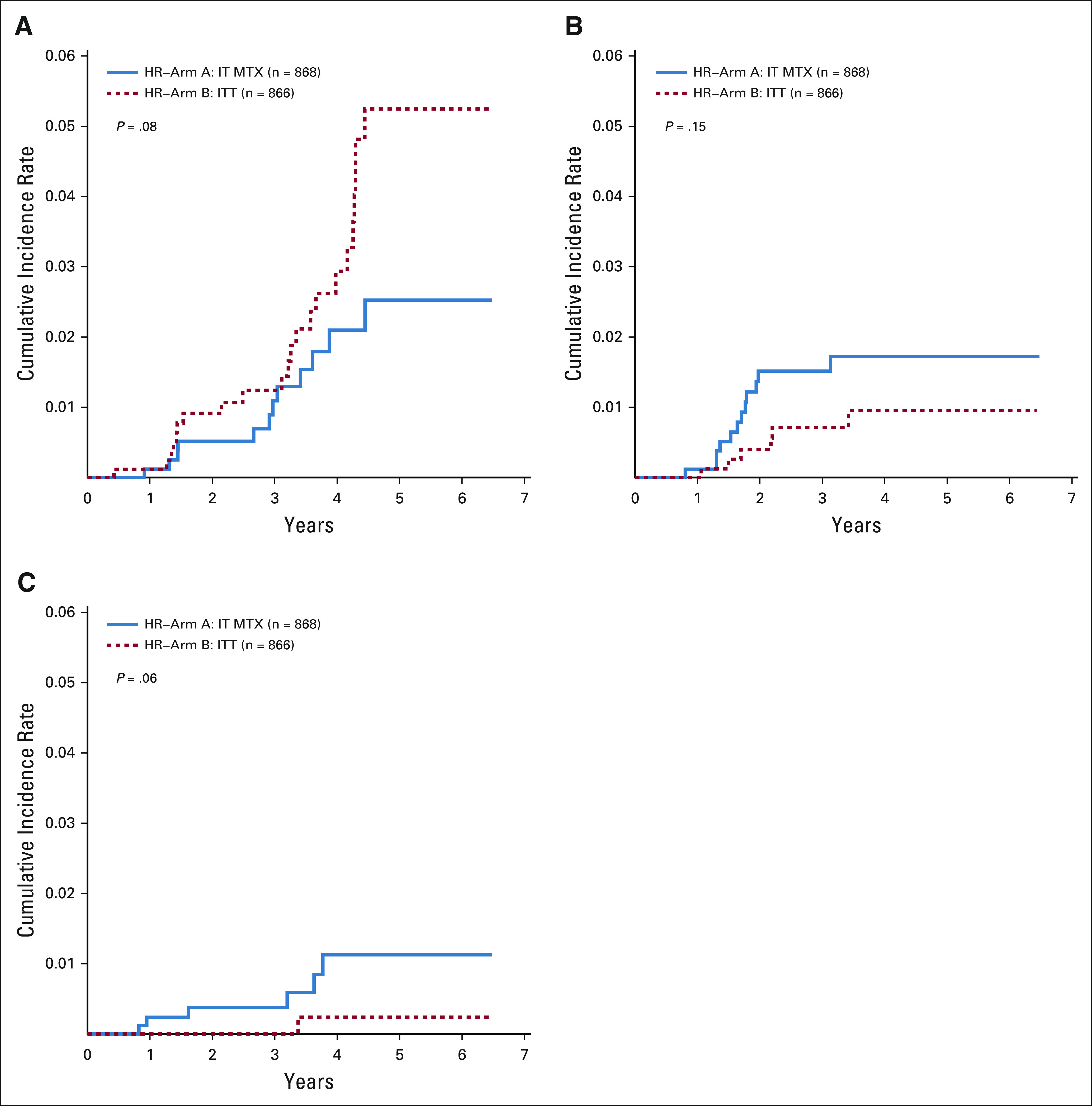
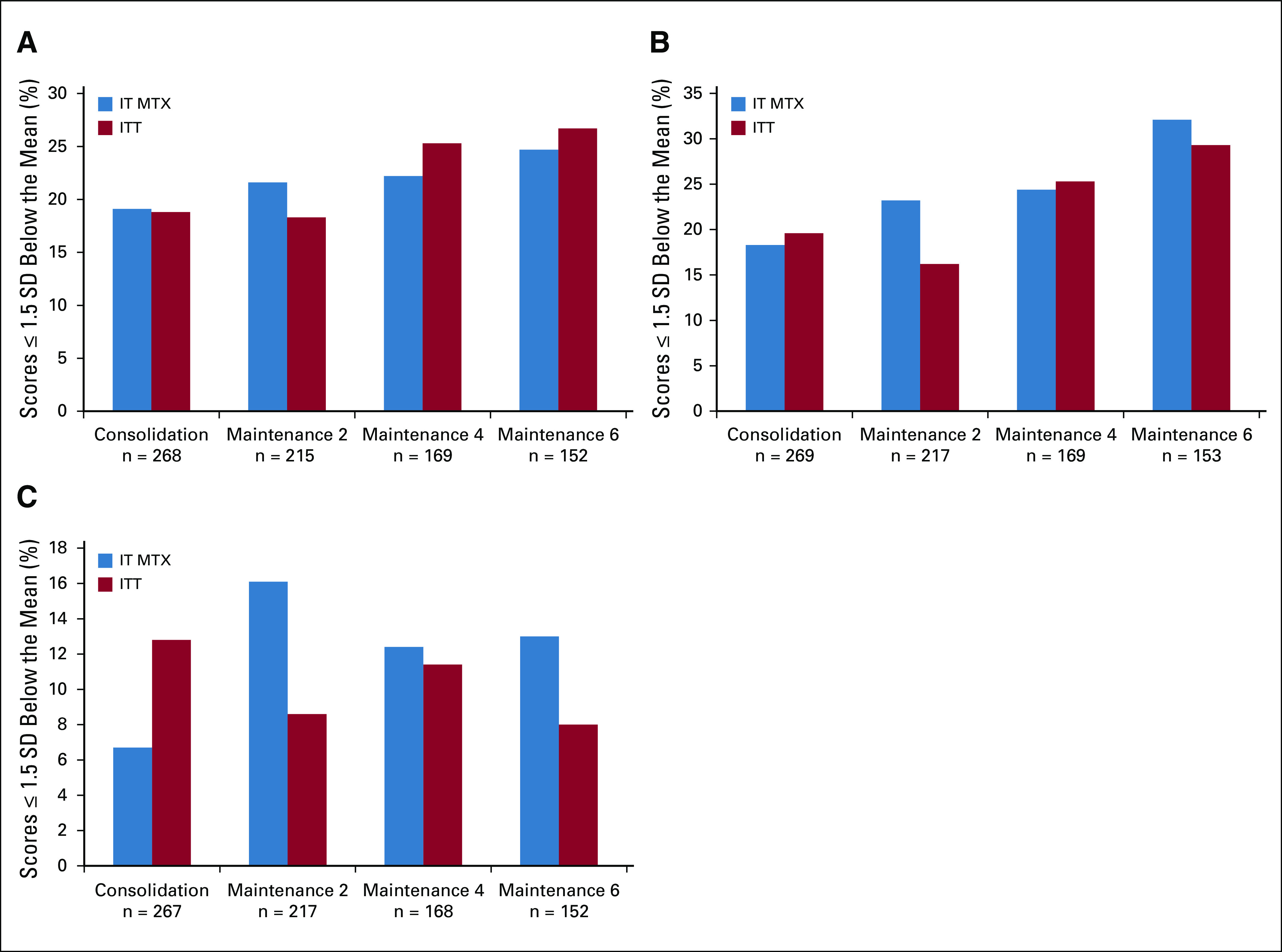
Results: Random assignment was closed to accrual in March 2018 after a futility boundary had been crossed, concluding that ITT could not be shown to be superior to IT MTX. The 5-year postinduction DFS and overall survival rates (± SE) of children randomly assigned to IT MTX versus ITT were 93.2% ± 2.1% v 90.6% ± 2.3% (P = .85), and 96.3% ± 1.5% v 96.7% ± 1.4% (P = .77), respectively. There were no differences in the cumulative incidence of isolated bone marrow relapse, isolated CNS relapse, or combined bone marrow and CNS relapse rates, or in toxicities observed for patients receiving IT MTX compared with ITT. There were no significant differences in neurocognitive outcomes for patients receiving IT MTX compared with ITT.
Conclusion: Postinduction CNS prophylaxis with ITT did not improve 5-year DFS for children with HR B-ALL. The standard of care for CNS prophylaxis for children with B-ALL and no overt CNS involvement remains IT MTX.
Trial registration: ClinicalTrials.gov NCT02883049.
Figures
References
-
- Möricke A, Zimmermann M, Reiter A, et al. Long-term results of five consecutive trials in childhood acute lymphoblastic leukemia performed by the ALL-BFM study group from 1981 to 2000. Leukemia. 2010;24:265–284. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
