

Importance of Genetic Studies of Cardiometabolic Disease in Diverse Populations
- PMID: 32496918
- PMCID: PMC7285892
- DOI: 10.1161/CIRCRESAHA.120.315893
Importance of Genetic Studies of Cardiometabolic Disease in Diverse Populations
Abstract
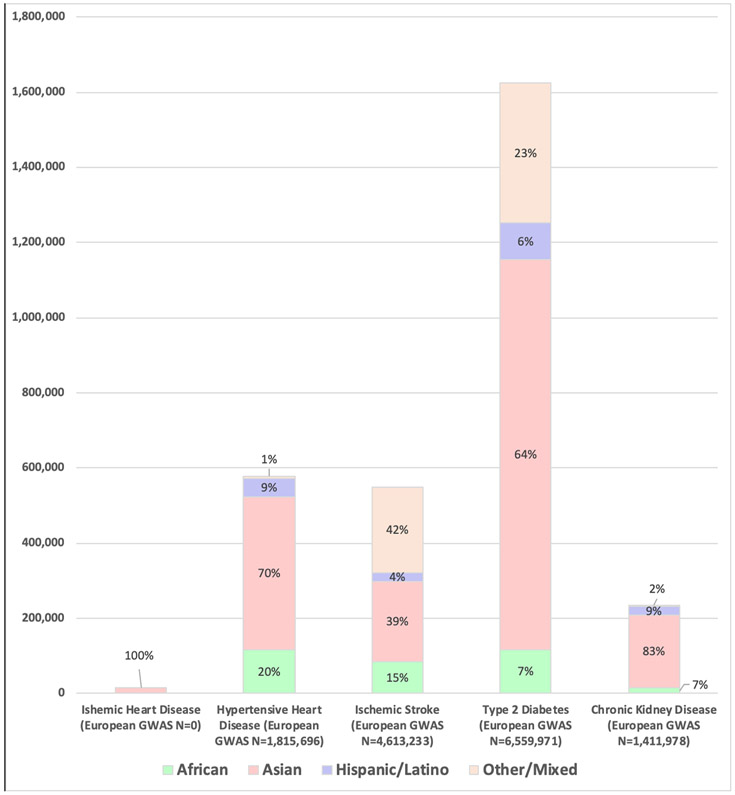
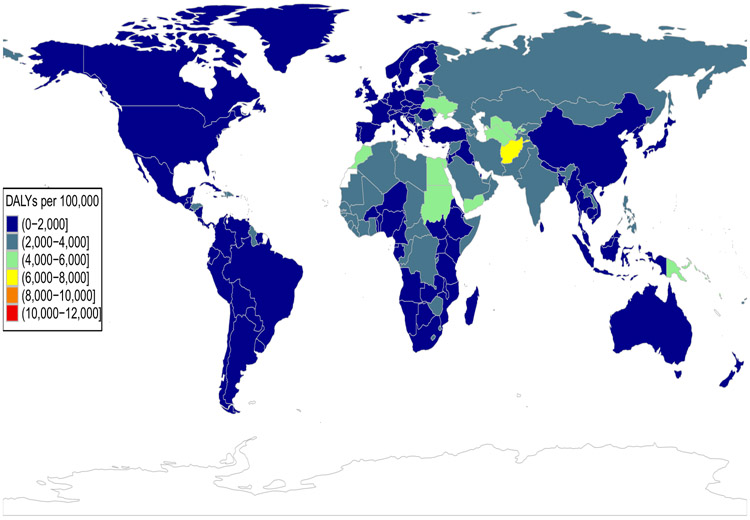
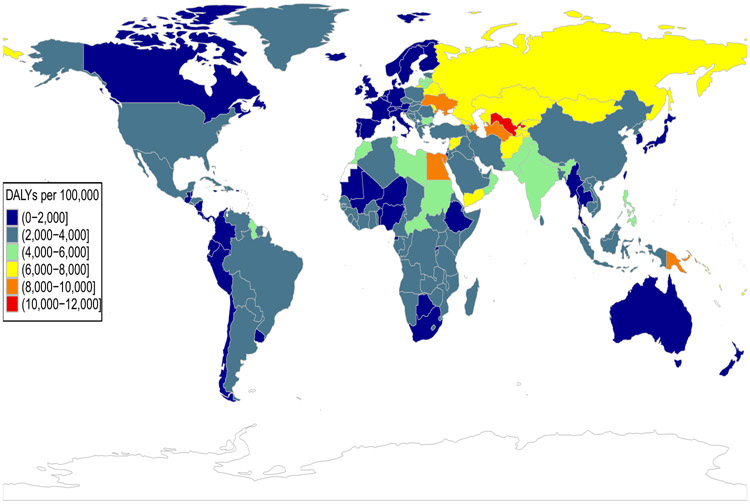
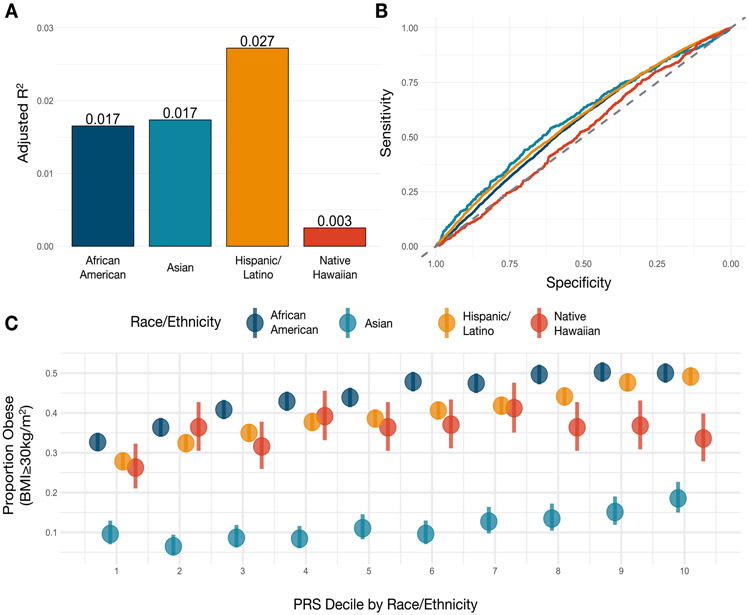
Genome-wide association studies have revolutionized our understanding of the genetic underpinnings of cardiometabolic disease. Yet, the inadequate representation of individuals of diverse ancestral backgrounds in these studies may undercut their ultimate potential for both public health and precision medicine. The goal of this review is to describe the imperativeness of studying the populations who are most affected by cardiometabolic disease, to the aim of better understanding the genetic underpinnings of the disease. We support this premise by describing the current variation in the global burden of cardiometabolic disease and emphasize the importance of building a globally and ancestrally representative genetics evidence base for the identification of population-specific variants, fine-mapping, and polygenic risk score estimation. We discuss the important ethical, legal, and social implications of increasing ancestral diversity in genetic studies of cardiometabolic disease and the challenges that arise from the (1) lack of diversity in current reference populations and available analytic samples and the (2) unequal generation of health-associated genomic data and their prediction accuracies. Despite these challenges, we conclude that additional, unprecedented opportunities lie ahead for public health genomics and the realization of precision medicine, provided that the gap in diversity can be systematically addressed. Achieving this goal will require concerted efforts by social, academic, professional and regulatory stakeholders and communities, and these efforts must be based on principles of equity and social justice.
Keywords: cardiovascular diseases; genomics; global burden of disease; metabolic diseases; minority health; precision medicine; social justice.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
