

Exploration of the effects of the CYCLOPS gene RBM17 in hepatocellular carcinoma
- PMID: 32497093
- PMCID: PMC7272028
- DOI: 10.1371/journal.pone.0234062
Exploration of the effects of the CYCLOPS gene RBM17 in hepatocellular carcinoma
Abstract
Background: Hepatocellular carcinoma (HCC) is one of the most lethal and malignant tumours worldwide. New therapeutic targets for HCC are urgently needed. CYCLOPS (copy number alterations yielding cancer liabilities owing to partial loss) genes have been noted to be associated with cancer-targeted therapies. Therefore, we intended to explore the effects of the CYCLOPS gene RBM17 on HCC oncogenesis to determine if it could be further used for targeted therapy.
Methods: We collected data on 12 types of cancer from the Cancer Genome Atlas (TCGA) and Gene Expression Omnibus (GEO) queries for comparison with adjacent non-tumour tissues. RBM17 expression levels, clinicopathological factors and survival times were analysed. RNAseq data were downloaded from the Encyclopaedia of DNA Elements database for molecular mechanism exploration. Two representative HCC cell models were built to observe the proliferation capacity of HCC cells when RBM17 expression was inhibited by shRBM17. Cell cycle progression and apoptosis were also examined to investigate the pathogenesis of RBM17.
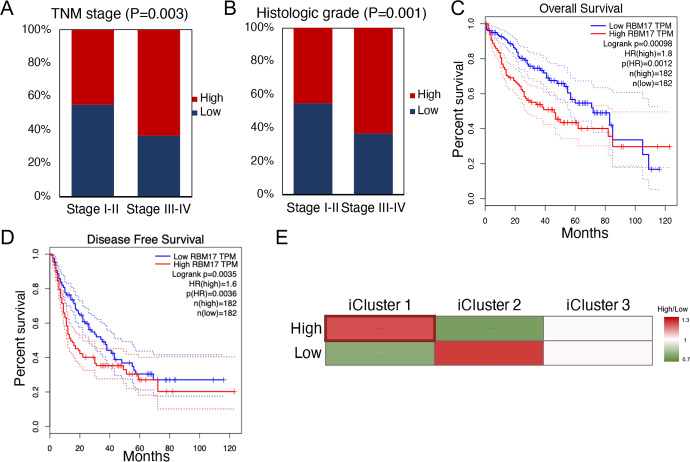
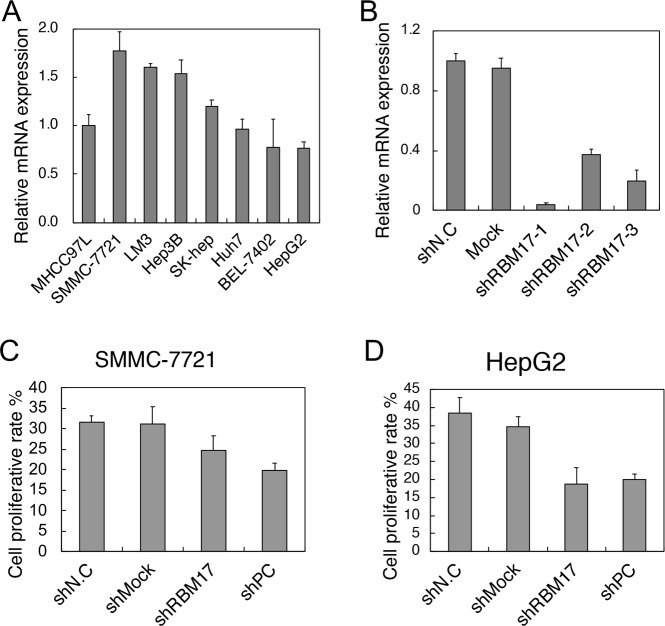
Results: Based on 6,136 clinical samples, RBM17 was markedly overexpressed in most cancers, especially HCC. Moreover, data from 442 patients revealed that high RBM17 expression levels were related to a worse prognosis. Overexpression of RBM17 was related to the iCluster1 molecular subgroup, TNM stage, and histologic grade. Pathway analysis of RNAseq data suggested that RBM17 was involved in mitosis. Further investigation revealed that the proliferation rates of HepG2 (P = 0.003) and SMMC-7721 (P = 0.030) cells were significantly reduced when RBM17 was knocked down. In addition, RBM17 knockdown also arrested the progression of the cell cycle, causing cells to halt at the G2/M phase. Increased apoptosis rates were also found in vitro.
Conclusion: These results suggest that RBM17 is a potential therapeutic target for HCC treatment.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures



References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
