

Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: a systematic review and meta-analysis
- PMID: 32497510
- PMCID: PMC7263814
- DOI: 10.1016/S0140-6736(20)31142-9
Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: a systematic review and meta-analysis
Abstract
Background: Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) causes COVID-19 and is spread person-to-person through close contact. We aimed to investigate the effects of physical distance, face masks, and eye protection on virus transmission in health-care and non-health-care (eg, community) settings.
Methods: We did a systematic review and meta-analysis to investigate the optimum distance for avoiding person-to-person virus transmission and to assess the use of face masks and eye protection to prevent transmission of viruses. We obtained data for SARS-CoV-2 and the betacoronaviruses that cause severe acute respiratory syndrome, and Middle East respiratory syndrome from 21 standard WHO-specific and COVID-19-specific sources. We searched these data sources from database inception to May 3, 2020, with no restriction by language, for comparative studies and for contextual factors of acceptability, feasibility, resource use, and equity. We screened records, extracted data, and assessed risk of bias in duplicate. We did frequentist and Bayesian meta-analyses and random-effects meta-regressions. We rated the certainty of evidence according to Cochrane methods and the GRADE approach. This study is registered with PROSPERO, CRD42020177047.
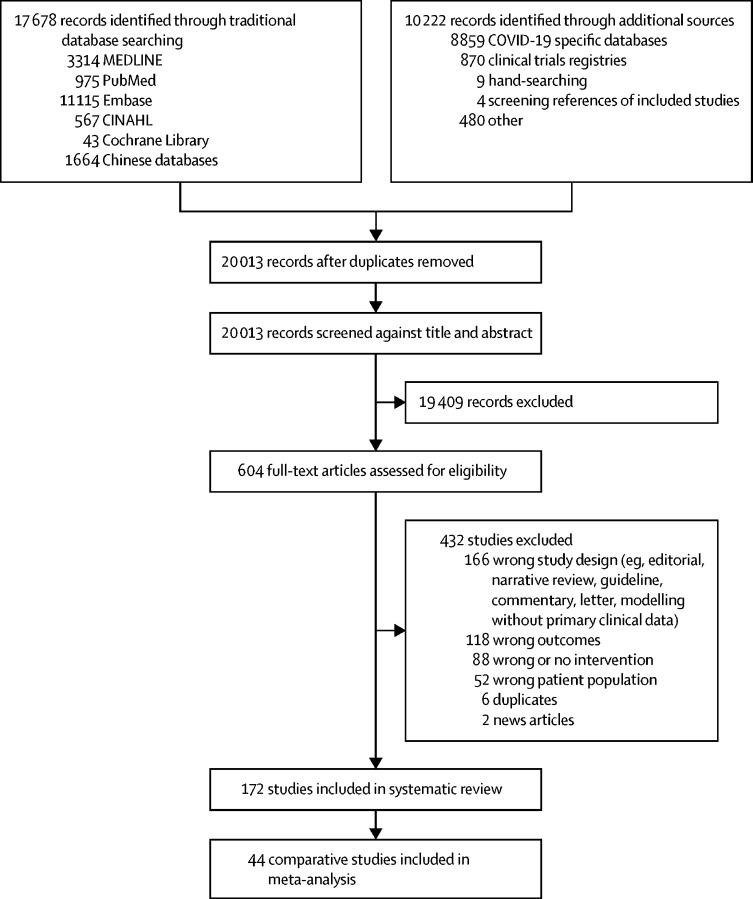
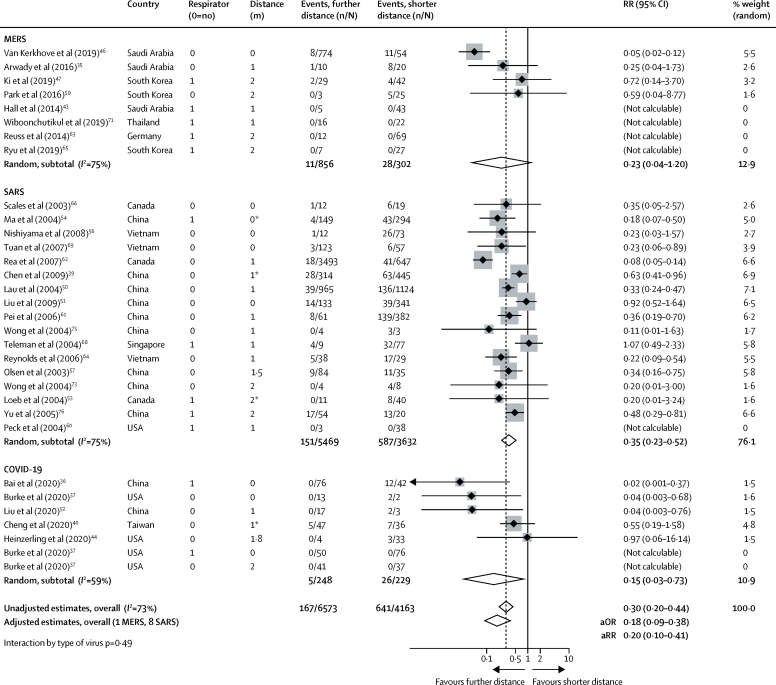
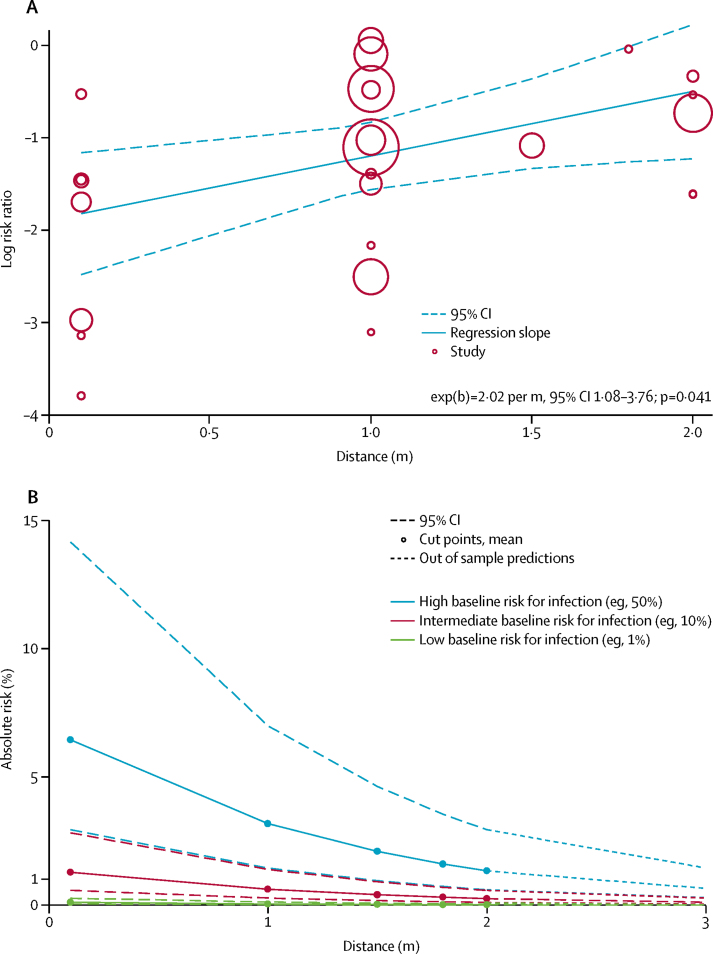
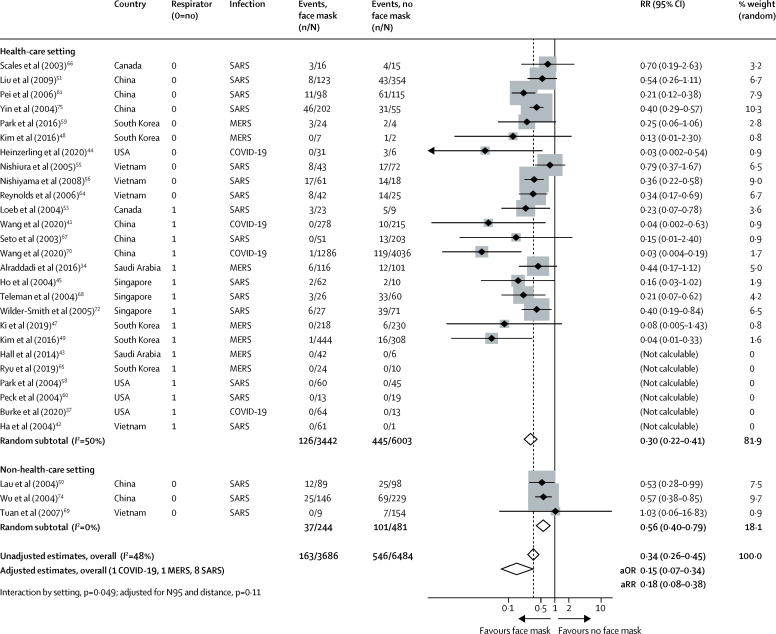
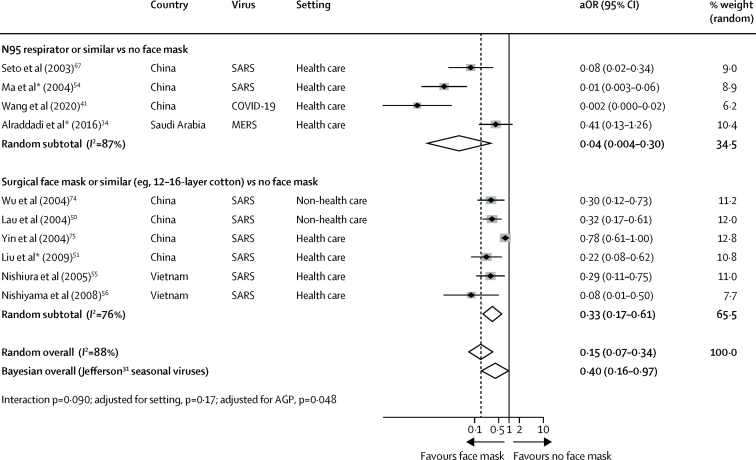
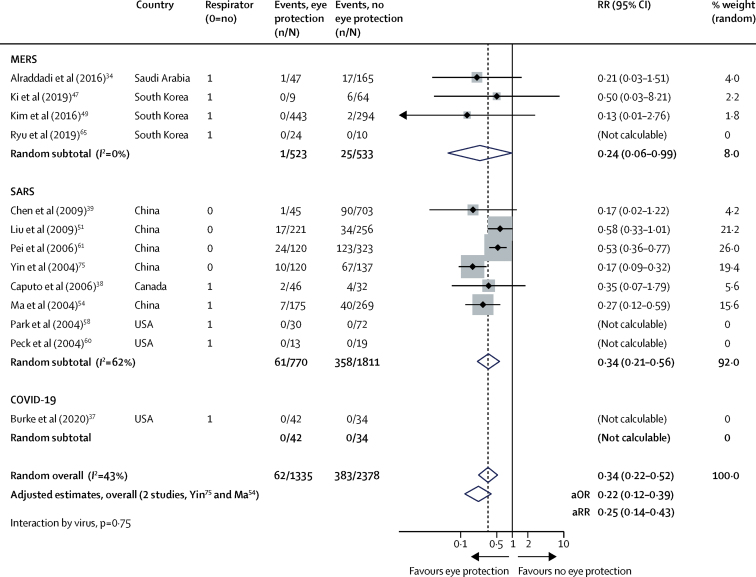
Findings: Our search identified 172 observational studies across 16 countries and six continents, with no randomised controlled trials and 44 relevant comparative studies in health-care and non-health-care settings (n=25 697 patients). Transmission of viruses was lower with physical distancing of 1 m or more, compared with a distance of less than 1 m (n=10 736, pooled adjusted odds ratio [aOR] 0·18, 95% CI 0·09 to 0·38; risk difference [RD] -10·2%, 95% CI -11·5 to -7·5; moderate certainty); protection was increased as distance was lengthened (change in relative risk [RR] 2·02 per m; pinteraction=0·041; moderate certainty). Face mask use could result in a large reduction in risk of infection (n=2647; aOR 0·15, 95% CI 0·07 to 0·34, RD -14·3%, -15·9 to -10·7; low certainty), with stronger associations with N95 or similar respirators compared with disposable surgical masks or similar (eg, reusable 12-16-layer cotton masks; pinteraction=0·090; posterior probability >95%, low certainty). Eye protection also was associated with less infection (n=3713; aOR 0·22, 95% CI 0·12 to 0·39, RD -10·6%, 95% CI -12·5 to -7·7; low certainty). Unadjusted studies and subgroup and sensitivity analyses showed similar findings.
Interpretation: The findings of this systematic review and meta-analysis support physical distancing of 1 m or more and provide quantitative estimates for models and contact tracing to inform policy. Optimum use of face masks, respirators, and eye protection in public and health-care settings should be informed by these findings and contextual factors. Robust randomised trials are needed to better inform the evidence for these interventions, but this systematic appraisal of currently best available evidence might inform interim guidance.
Funding: World Health Organization.
© 2020 World Health Organization. Published by Elsevier Ltd. This is an Open Access article published under the CC BY 3.0 IGO license which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. In any use of this article, there should be no suggestion that WHO endorses any specific organisation, products or services. The use of the WHO logo is not permitted. This notice should be preserved along with the article's original URL.
Figures
Comment in
-
Physical distancing, face masks, and eye protection for prevention of COVID-19.Lancet. 2020 Jun 27;395(10242):1950-1951. doi: 10.1016/S0140-6736(20)31183-1. Epub 2020 Jun 1. Lancet. 2020. PMID: 32497511 Free PMC article. No abstract available.
-
COVID-19 and the personal protection debate: An exposition on transmission.J Paediatr Child Health. 2020 Sep;56(9):1486. doi: 10.1111/jpc.15054. Epub 2020 Jul 6. J Paediatr Child Health. 2020. PMID: 32628312 Free PMC article. No abstract available.
-
The cumulative risk of acquiring COVID-19 in outpatient pediatric practice.Pediatr Pulmonol. 2021 Jan;56(1):19-20. doi: 10.1002/ppul.25144. Epub 2020 Nov 19. Pediatr Pulmonol. 2021. PMID: 33210837 Free PMC article. No abstract available.
-
Double-zero-event studies matter: A re-evaluation of physical distancing, face masks, and eye protection for preventing person-to-person transmission of COVID-19 and its policy impact.J Clin Epidemiol. 2021 May;133:158-160. doi: 10.1016/j.jclinepi.2021.01.021. Epub 2021 Feb 2. J Clin Epidemiol. 2021. PMID: 33539929 Free PMC article. No abstract available.
-
Restrictions related to COVID-19 can negatively affect Russian patients with chronic spontaneous urticaria.Eur Ann Allergy Clin Immunol. 2023 Mar;55(2):94-96. doi: 10.23822/EurAnnACI.1764-1489.226. Epub 2021 Jul 21. Eur Ann Allergy Clin Immunol. 2023. PMID: 34284569 No abstract available.
-
Revisiting the evidence for physical distancing, face masks, and eye protection.Lancet. 2021 Aug 21;398(10301):659-660. doi: 10.1016/S0140-6736(21)01742-6. Lancet. 2021. PMID: 34419197 Free PMC article. No abstract available.
-
Revisiting the evidence for physical distancing, face masks, and eye protection.Lancet. 2021 Aug 21;398(10301):660. doi: 10.1016/S0140-6736(21)01741-4. Lancet. 2021. PMID: 34419198 Free PMC article. No abstract available.
-
Revisiting the evidence for physical distancing, face masks, and eye protection.Lancet. 2021 Aug 21;398(10301):660-661. doi: 10.1016/S0140-6736(21)01736-0. Lancet. 2021. PMID: 34419199 Free PMC article. No abstract available.
-
Revisiting the evidence for physical distancing, face masks, and eye protection.Lancet. 2021 Aug 21;398(10301):661-663. doi: 10.1016/S0140-6736(21)01739-6. Lancet. 2021. PMID: 34419200 Free PMC article. No abstract available.
-
Revisiting the evidence for physical distancing, face masks, and eye protection.Lancet. 2021 Aug 21;398(10301):661. doi: 10.1016/S0140-6736(21)01738-4. Lancet. 2021. PMID: 34419201 Free PMC article. No abstract available.
-
Revisiting the evidence for physical distancing, face masks, and eye protection.Lancet. 2021 Aug 21;398(10301):663. doi: 10.1016/S0140-6736(21)01758-X. Lancet. 2021. PMID: 34419203 Free PMC article. No abstract available.
-
Kommentar zu „Welchen Stellenwert haben Abstand, Masken und Augenschutz bei SARS-CoV2?“.Laryngorhinootologie. 2021 Oct;100(10):769-770. doi: 10.1055/a-1500-5269. Epub 2021 Oct 6. Laryngorhinootologie. 2021. PMID: 34614522 German. No abstract available.
-
Welchen Stellenwert haben Abstand, Masken und Augenschutz bei SARS-CoV2?Laryngorhinootologie. 2021 Oct;100(10):769. doi: 10.1055/a-1623-9504. Epub 2021 Oct 6. Laryngorhinootologie. 2021. PMID: 34614523 German. No abstract available.
References
-
- Worldometer COVID-19 coronavirus pandemic. 2020. https://www.worldometers.info/coronavirus/
-
- Chia PY, Coleman KK, Tan YK. Detection of air and surface contamination by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in hospital rooms of infected patients. medRxiv. 2020 doi: 10.1101/2020.03.29.20046557. published online April 9. (preprint). - DOI
-
- Santarpia JL, Rivera DN, Herrera V. Transmission potential of SARS-CoV-2 in viral shedding observed at the University of Nebraska Medical Center. medRxiv. 2020 doi: 10.1101/2020.03.23.20039446. published online March 26. (preprint). - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
