

Effects of Different Types of Exercise Training on Pulmonary Arterial Hypertension: A Systematic Review
- PMID: 32498263
- PMCID: PMC7356848
- DOI: 10.3390/jcm9061689
Effects of Different Types of Exercise Training on Pulmonary Arterial Hypertension: A Systematic Review
Abstract
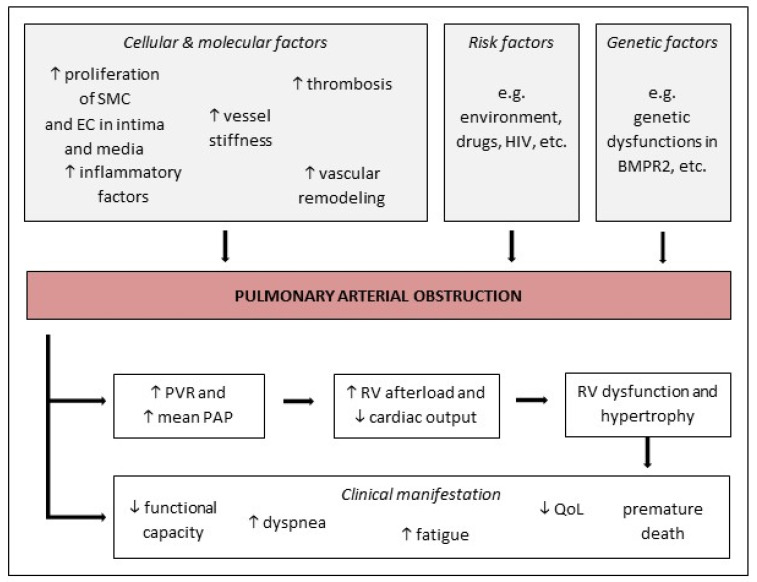
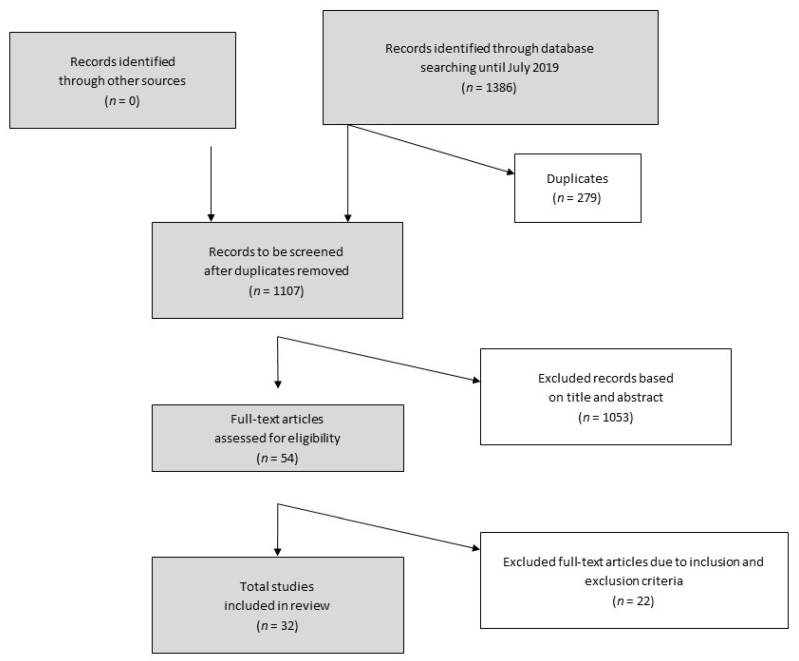
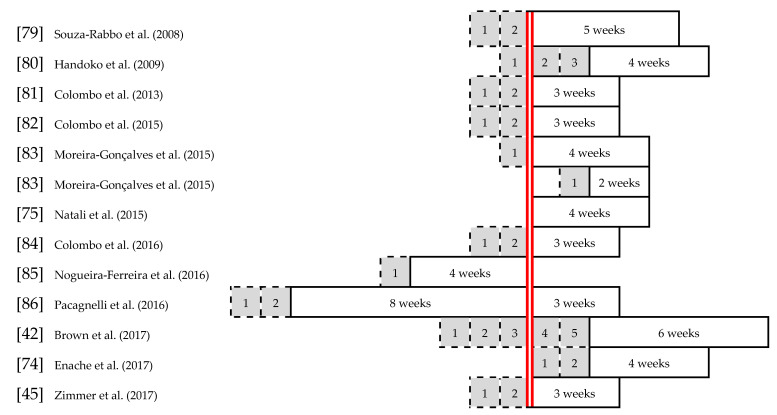
Pulmonary arterial hypertension (PAH) represents a chronic progressive disease characterized by high blood pressure in the pulmonary arteries leading to right heart failure. The disease has been a focus of medical research for many years due to its worse prognosis and limited treatment options. The aim of this study was to systematically assess the effects of different types of exercise interventions on PAH. Electronic databases were searched until July 2019. MEDLINE database was used as the predominant source for this paper. Studies with regards to chronic physical activity in adult PAH patients are compared on retrieving evidence on cellular, physiological, and psychological alterations in the PAH setting. Twenty human studies and 12 rat trials were identified. Amongst all studies, a total of 628 human subjects and 614 rats were examined. Regular physical activity affects the production of nitric oxygen and attenuates right ventricular hypertrophy. A combination of aerobic, anaerobic, and respiratory muscle training induces the strongest improvement in functional capacity indicated by an increase of 6 MWD and VO2peak. In human studies, an increase of quality of life was found. Exercise training has an overall positive effect on the physiological and psychological components of PAH. Consequently, PAH patients should be encouraged to take part in regular exercise training programs.
Keywords: exercise training; experimental models; human studies; pulmonary arterial hypertension.
Conflict of interest statement
The authors declare no conflicts of interests regarding the publication of this manuscript.
Figures
References
-
- Galiè N., Humbert M., Vachiery J.-L., Gibbs S., Lang I., Torbicki A., Simonneau G., Peacock A., Vonk Noordegraaf A., Beghetti M., et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT) Eur. Heart J. 2016;37:67–119. doi: 10.1093/eurheartj/ehv317. - DOI - PubMed
-
- Humbert M., Guignabert C., Bonnet S., Dorfmüller P., Klinger J.R., Nicolls M.R., Olschewski A.J., Pullamsetti S.S., Schermuly R.T., Stenmark K.R., et al. Pathology and pathobiology of pulmonary hypertension: State of the art and research perspectives. Eur. Respir. J. 2019;53 doi: 10.1183/13993003.01887-2018. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
