

The clinical and cost effectiveness of surgical interventions for stones in the lower pole of the kidney: the percutaneous nephrolithotomy, flexible ureterorenoscopy and extracorporeal shockwave lithotripsy for lower pole kidney stones randomised controlled trial (PUrE RCT) protocol
- PMID: 32498699
- PMCID: PMC7273687
- DOI: 10.1186/s13063-020-04326-x
The clinical and cost effectiveness of surgical interventions for stones in the lower pole of the kidney: the percutaneous nephrolithotomy, flexible ureterorenoscopy and extracorporeal shockwave lithotripsy for lower pole kidney stones randomised controlled trial (PUrE RCT) protocol
Abstract
Introduction: Renal stones are common, with a lifetime prevalence of 10% in adults. Global incidence is increasing due to increases in obesity and diabetes, with these patient populations being more likely to suffer renal stone disease. Flank pain from stones (renal colic) is the most common cause of emergency admission to UK urology departments. Stones most commonly develop in the lower pole of the kidney (in ~35% of cases) and here are least likely to pass without intervention. Currently there are three technologies available within the UK National Health Service to remove lower pole kidney stones: extracorporeal shockwave lithotripsy (ESWL), percutaneous nephrolithotomy (PCNL) and flexible ureterorenoscopy (FURS) with laser lithotripsy. Current evidence indicates there is uncertainty regarding the management of lower pole stones, and each treatment has advantages and disadvantages. The aim of this trial is to determine the clinical and cost effectiveness of FURS compared with ESWL or PCNL in the treatment of lower pole kidney stones.
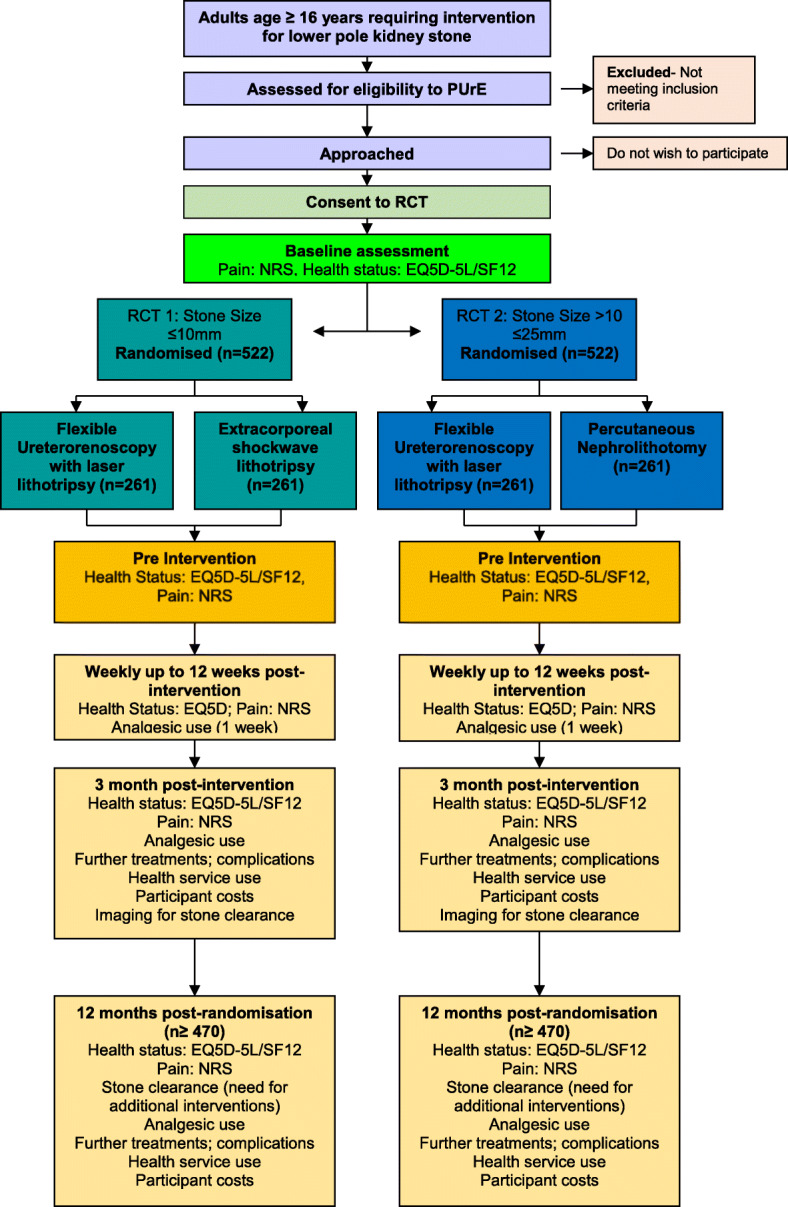
Methods: The PUrE (PCNL, FURS and ESWL for lower pole kidney stones) trial is a multi-centre, randomised controlled trial (RCT) evaluating FURS versus ESWL or PCNL for lower pole kidney stones. Patients aged ≥16 years with a stone(s) in the lower pole of either kidney confirmed by non-contrast computed tomography of the kidney, ureter and bladder (CTKUB) and requiring treatment for a stone ≤10 mm will be randomised to receive FURS or ESWL (RCT1), and those requiring treatment for a stone >10 mm to ≤25 mm will be randomised to receive FURS or PCNL (RCT2). Participants will undergo follow-up by questionnaires every week up to 12 weeks post-intervention and at 12 months post-randomisation. The primary clinical outcome is health status measured by the area under the curve calculated from multiple measurements of the EuroQol five dimensions five-level version (EQ-5D-5L) questionnaire up to 12 weeks post-intervention. The primary economic outcome is the incremental cost per quality-adjusted life year gained at 12 months post-randomisation.
Discussion: The PUrE trial aims to provide robust evidence on health status, quality of life, clinical outcomes and resource use to directly inform choice and National Health Service provision of the three treatment options.
Trial registration: ISRCTN: ISRCTN98970319. Registered on 11 November 2015.
Keywords: Extracorporeal shockwave lithotripsy; Flexible ureterorenoscopy; Lower pole stone; Percutaneous nephrolithotomy; Renal stone.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Clinical and cost-effectiveness of percutaneous nephrolithotomy, flexible ureterorenoscopy and extracorporeal shockwave lithotripsy for lower pole stones: the PUrE RCTs.Health Technol Assess. 2025 Aug;29(40):1-186. doi: 10.3310/WFRE6844. Health Technol Assess. 2025. PMID: 40823754 Free PMC article. Clinical Trial.
-
The PUrE randomised controlled trial 1: Clinical and cost effectiveness of flexible ureterorenoscopy and extracorporeal shockwave lithotripsy for lower pole stones of ≤10 mm.Eur Urol. 2025 Aug;88(2):179-189. doi: 10.1016/j.eururo.2025.02.002. Epub 2025 Apr 22. Eur Urol. 2025. PMID: 40268593 Clinical Trial.
-
Meta-analysis of Optimal Management of Lower Pole Stone of 10 - 20 mm: Flexible Ureteroscopy (FURS) versus Extracorporeal Shock Wave Lithotripsy (ESWL) versus Percutaneus Nephrolithotomy (PCNL).Acta Med Indones. 2018 Jan;50(1):18-25. Acta Med Indones. 2018. PMID: 29686172
-
Updated Systematic Review and Meta-analysis of Extracorporeal Shock Wave Lithotripsy, Flexible Ureterorenoscopy, and Percutaneous Nephrolithotomy for Lower Pole Renal Stones.Eur Urol. 2025 Sep;88(3):231-239. doi: 10.1016/j.eururo.2025.01.020. Epub 2025 Mar 13. Eur Urol. 2025. PMID: 40082136 Review.
-
Extracorporeal shockwave lithotripsy vs. percutaneous nephrolithotomy vs. flexible ureterorenoscopy for lower-pole stones.Arab J Urol. 2012 Sep;10(3):336-41. doi: 10.1016/j.aju.2012.06.004. Epub 2012 Jul 24. Arab J Urol. 2012. PMID: 26558046 Free PMC article. Review.
Cited by
-
[Stones in the lower pole and their treatment].Urologie. 2025 Jul;64(7):715-724. doi: 10.1007/s00120-025-02577-7. Epub 2025 Jun 23. Urologie. 2025. PMID: 40549000 German.
-
Clinical and cost-effectiveness of percutaneous nephrolithotomy, flexible ureterorenoscopy and extracorporeal shockwave lithotripsy for lower pole stones: the PUrE RCTs.Health Technol Assess. 2025 Aug;29(40):1-186. doi: 10.3310/WFRE6844. Health Technol Assess. 2025. PMID: 40823754 Free PMC article. Clinical Trial.
-
Endourological Options for Small (< 2 cm) Lower Pole Stones - Does the Lower Pole Angle Matter?Curr Urol Rep. 2023 Aug;24(8):365-370. doi: 10.1007/s11934-023-01161-w. Epub 2023 Apr 25. Curr Urol Rep. 2023. PMID: 37097431 Free PMC article. Review.
-
Clinical comparative study of standard channel percutaneous nephroscope combined with flexible ureteroscope and traditional standard channel combined with microchannel percutaneous nephrolithotomy in the treatment of multiple renal calculi without hydronephrosis.Pak J Med Sci. 2022 Sep-Oct;38(7):1844-1851. doi: 10.12669/pjms.38.7.5526. Pak J Med Sci. 2022. PMID: 36246701 Free PMC article.
-
Effect of infundibulopelvic angle on outcomes of ureteroscopy: a systematic review and meta-analysis.World J Urol. 2024 Jul 16;42(1):413. doi: 10.1007/s00345-024-05104-z. World J Urol. 2024. PMID: 39012390 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
