

Nodular pulmonary deposition disease in a patient with the acquired immunodeficiency syndrome: a case report
- PMID: 32498712
- PMCID: PMC7273682
- DOI: 10.1186/s13256-020-02394-w
Nodular pulmonary deposition disease in a patient with the acquired immunodeficiency syndrome: a case report
Abstract
Background: Pulmonary nodules are a common cause for concern in patients with human immunodeficiency virus and acquired immunodeficiency syndrome. Most commonly, they are the result of an infection, given the patients' immunocompromised state; however, in some cases, pulmonary nodules in patients with human immunodeficiency virus and patients with acquired immunodeficiency syndrome can result from cellular or protein deposits. We report a rare case of nodular pulmonary light chain deposition disease in a patient with acquired immunodeficiency syndrome and monoclonal gammopathy of undetermined significance.
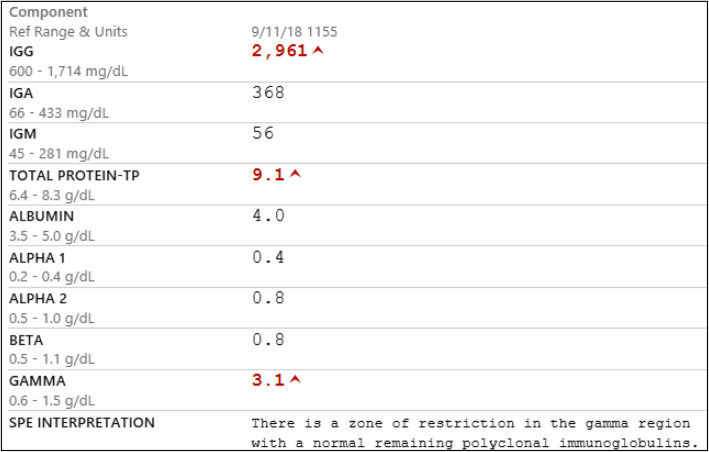
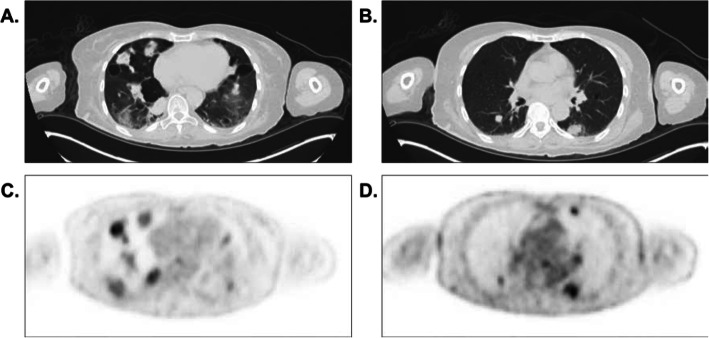
Case presentation: A 53-year-old African American woman with acquired immunodeficiency syndrome had pulmonary nodules detected incidentally by imaging of her lungs. Pulmonary tuberculosis was high on the differential diagnosis, but she had a negative test result for pulmonary tuberculosis. Imaging also revealed multiple lucent bone lesions, and earlier in the year, serum protein electrophoresis had shown an immunoglobulin G-kappa monoclonal protein (M spike). She was mildly anemic, so there was concern for progression to myeloma; however, the result of her bone marrow biopsy was unremarkable. Lung biopsy revealed finely granular eosinophilic material with negative Congo red staining, consistent with light chain deposition disease.
Conclusions: The extent of this patient's light chain deposition disease was thought to be caused by a combination of acquired immunodeficiency syndrome and monoclonal gammopathy of undetermined significance, and the interval decrease in lung nodule size after restarting antiretroviral therapy confirms this hypothesis and also highlights a potentially unique contribution of the hypergammaglobulinemia to this disease process in patients with human immunodeficiency virus and patients with acquired immunodeficiency syndrome .
Keywords: AIDS; HIV; Hypergammaglobulinemia; Light chain deposition disease (LCDD).
Conflict of interest statement
The authors have no competing interests to disclose.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
