

Conscious Sedation Versus General Anesthesia for Transcatheter Aortic Valve Replacement: Variation in Practice and Outcomes
- PMID: 32499018
- PMCID: PMC7650030
- DOI: 10.1016/j.jcin.2020.03.008
Conscious Sedation Versus General Anesthesia for Transcatheter Aortic Valve Replacement: Variation in Practice and Outcomes
Abstract
Objectives: The aims of this study were to examine variation in the use of conscious sedation (CS) for transcatheter aortic valve replacement (TAVR) across hospitals and over time and to evaluate outcomes of CS compared with general anesthesia (GA) using instrumental variable analysis, a quasi-experimental method to control for unmeasured confounding.
Background: Despite increasing use of CS for TAVR, contemporary data on utilization patterns are lacking, and existing studies evaluating the impact of sedation choice on outcomes may suffer from unmeasured confounding.
Methods: Among 120,080 patients in the TVT (Transcatheter Valve Therapy) Registry who underwent transfemoral TAVR between January 2016 and March 2019, the relationship between anesthesia choice and TAVR outcomes was evaluated using hospital proportional use of CS as an instrumental variable.
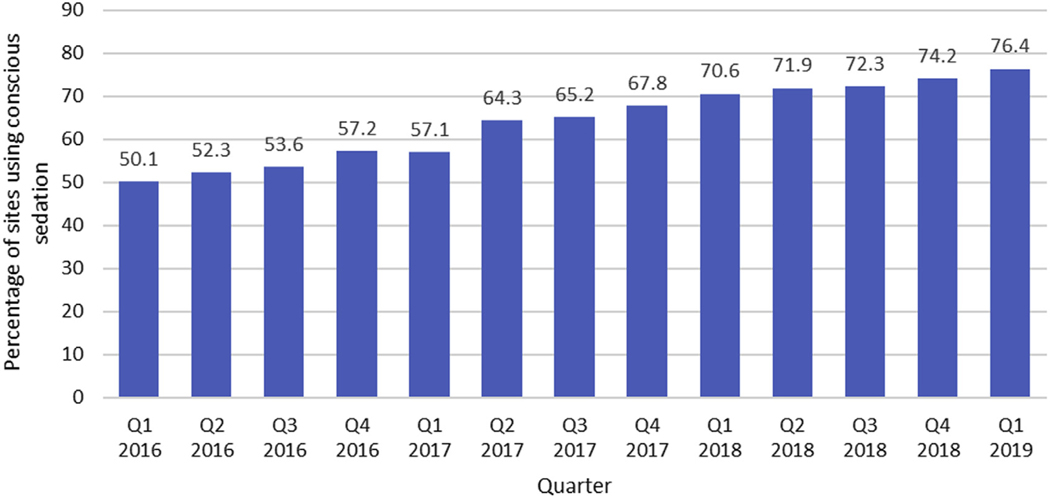
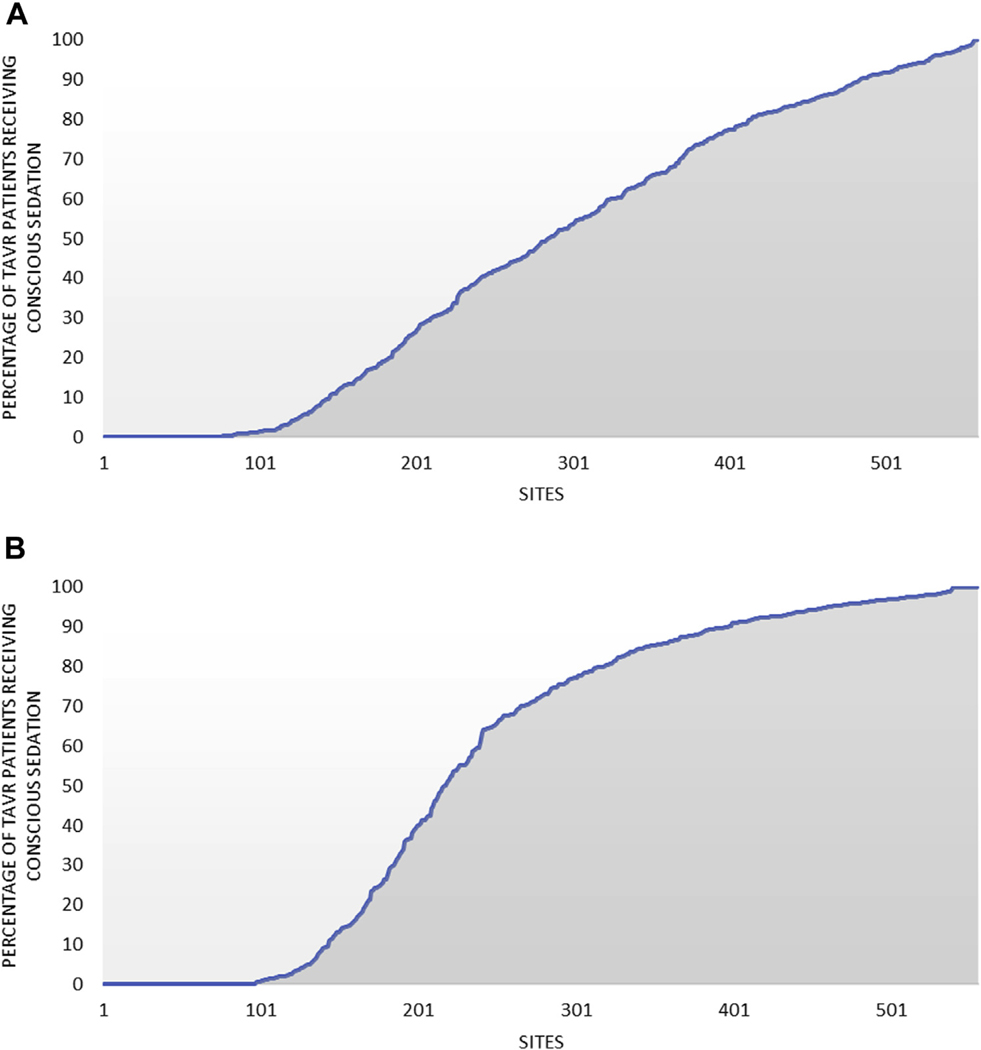
Results: Over the study period, the proportion of TAVR performed using CS increased from 33% to 64%, and CS was used in a median of 0% and 91% of cases in the lowest and highest quartiles of hospital CS use, respectively. On the basis of instrumental variable analysis, CS was associated with decreases in in-hospital mortality (adjusted risk difference: 0.2%; p = 0.010) and 30-day mortality (adjusted risk difference: 0.5%; p < 0.001), shorter length of hospital stay (adjusted difference: 0.8 days; p < 0.001), and more frequent discharge to home (adjusted risk difference: 2.8%; p < 0.001) compared with GA. The magnitude of benefit for most endpoints was less than in a traditional propensity score-based approach, however.
Conclusions: In contemporary U.S. practice, the use of CS for TAVR continues to increase, although there remains wide variation across hospitals. The use of CS for TAVR is associated with improved outcomes (including reduced mortality) compared with GA, although the magnitude of benefit appears to be less than in previous studies.
Keywords: TAVR; anesthesia; aortic stenosis; outcomes; variation.
Copyright © 2020 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures

Comment in
-
Transfemoral Transcatheter Aortic Valve Replacement: Conscious Sedation for Everyone?JACC Cardiovasc Interv. 2020 Jun 8;13(11):1288-1290. doi: 10.1016/j.jcin.2020.03.043. JACC Cardiovasc Interv. 2020. PMID: 32499019 No abstract available.
References
-
- Cribier A, Eltchaninoff H, Bash A, et al. Percutaneous transcatheter implantation of an aortic valve prosthesis for calcific aortic stenosis: first human case description. Circulation 2002;106: 3006–8. - PubMed
-
- Wood DA, Lauck SB, Cairns JA, et al. The Vancouver 3M (Multidisciplinary, Multimodality, but Minimalist) clinical pathway facilitates safe next-day discharge home at low-, medium-, and high-volume transfemoral transcatheter aortic valve replacement centers: the 3M TAVR study. J Am Coll Cardiol Intv 2019;12:459–69. - PubMed
-
- Attizzani GF, Patel SM, Dangas GD, et al. Comparison of local versus general anesthesia following transfemoral transcatheter self-expanding aortic valve implantation (from the Transcatheter Valve Therapeutics Registry). Am J Cardiol 2019;123:419–25. - PubMed
-
- Hyman MC, Vemulapalli S, Szeto WY, et al. Conscious sedation versus general anesthesia for transcatheter aortic valve replacement: insights from the National Cardiovascular Data Registry Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Therapy Registry. Circulation 2017;136:2132–40. - PubMed
-
- Thiele H. A 2×2 randomized trial of self-expandable vs balloon-expandable valves and general vs local anesthesia in patients undergoing transcatheter aortic valve implantation. Presented at: Transcatheter Cardiovascular Therapeutics; 2018; San Diego, CA.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
