

Combination of Oral Anticoagulants and Single Antiplatelets versus Triple Therapy in Nonvalvular Atrial Fibrillation and Acute Coronary Syndrome: Stroke Prevention among Asians
- PMID: 32499669
- PMCID: PMC7253348
- DOI: 10.1055/s-0040-1708477
Combination of Oral Anticoagulants and Single Antiplatelets versus Triple Therapy in Nonvalvular Atrial Fibrillation and Acute Coronary Syndrome: Stroke Prevention among Asians
Abstract
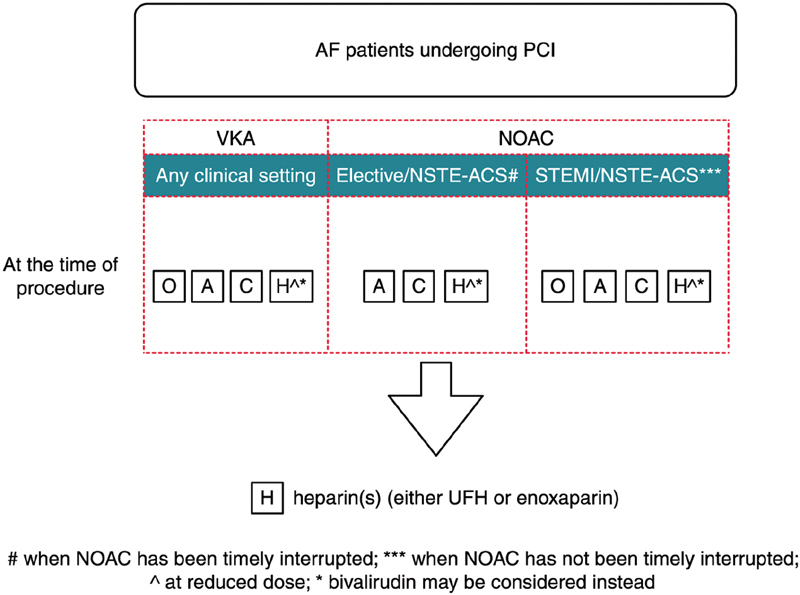
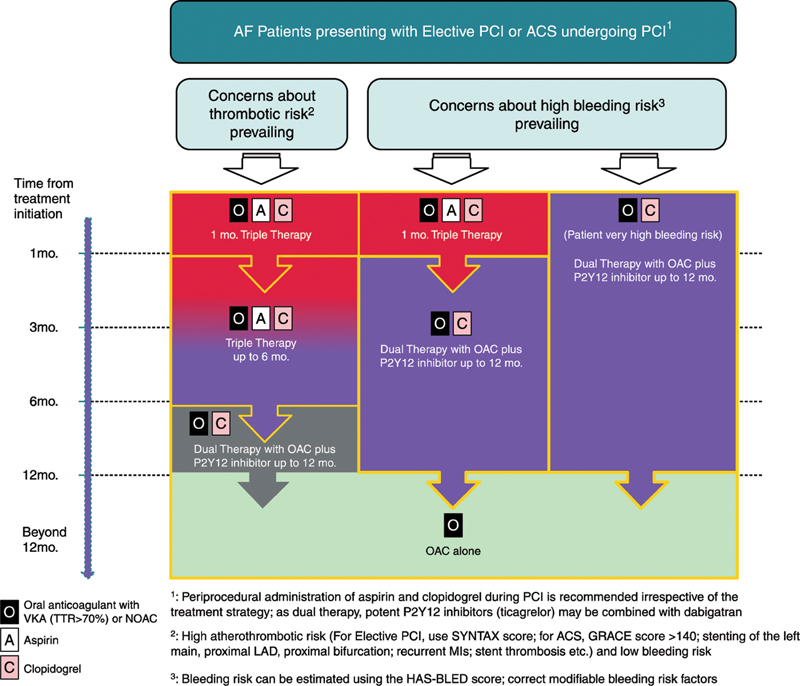
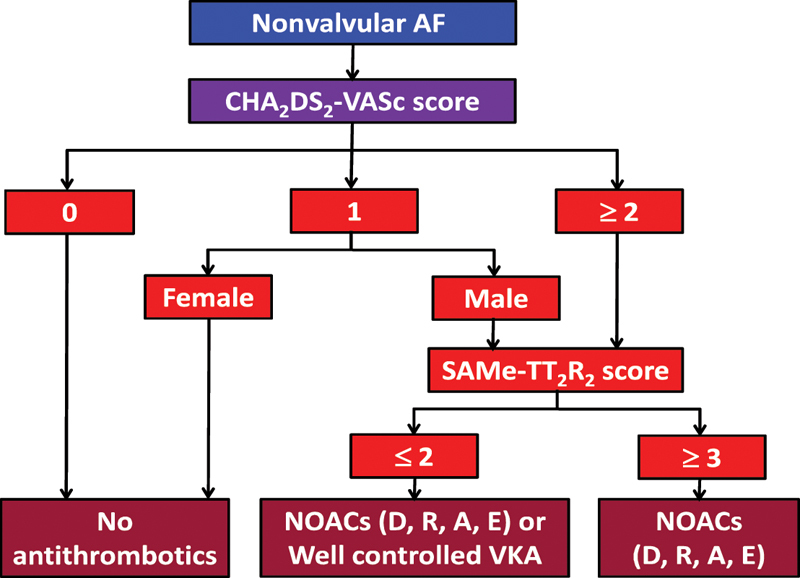
Atrial fibrillation (AF), the most prevalent arrhythmic disease, tends to foster thrombus formation due to hemodynamic disturbances, leading to severe disabling and even fatal thromboembolic diseases. Meanwhile, patients with AF may also present with acute coronary syndrome (ACS) and coronary artery disease (CAD) requiring stenting, which creates a clinical dilemma considering that majority of such patients will likely receive oral anticoagulants (OACs) for stroke prevention and require additional double antiplatelet treatment (DAPT) to reduce recurrent cardiac events and in-stent thrombosis. In such cases, the gentle balance between bleeding risk and atherothromboembolic events needs to be carefully considered. Studies have shown that congestive heart failure, hypertension, age ≥ 75 years (doubled), diabetes mellitus, and previous stroke or transient ischemic attack (TIA; doubled)-vascular disease, age 65 to 74 years, sex category (female; CHA 2 DS 2 -VASc) scores outperform other scoring systems in Asian populations and that the hypertension, abnormal renal/liver function (1 point each), stroke, bleeding history or predisposition, labile international normalized ratio (INR), elderly (>65 years), drugs/alcohol concomitantly (1 point each; HAS-BLED) score, a simple clinical score that predicts bleeding risk in patients with AF, particularly among Asians, performs better than other bleeding scores. A high HAS-BLED score should not be used to rule out OAC treatment but should instead prompt clinicians to address correctable risk factors. Therefore, the current review attempted to analyze available data from patients with nonvalvular AF who underwent stenting for ACS or CAD and elaborate on the direct-acting oral anticoagulant (DOAC) and antiplatelet management among such patients. For majority of the patients, "triple therapy" comprising OAC, aspirin, and clopidogrel should be considered for 1 to 6 months following ACS. However, the optimal duration for "triple therapy" would depend on the patient's ischemic and bleeding risks, with DOACs being obviously safer than vitamin-K antagonists.
Keywords: acute coronary syndrome; antiplatelets; nonvalvular atrial fibrillation; oral anticoagulants; stroke; thromboembolic diseases; triple therapy.
© Thieme Medical Publishers.
Conflict of interest statement
Conflict of Interest The authors confirm that they have no conflicts of interest pertinent to this article.
Figures
Similar articles
-
The HAS-BLED score has better prediction accuracy for major bleeding than CHADS2 or CHA2DS2-VASc scores in anticoagulated patients with atrial fibrillation.J Am Coll Cardiol. 2013 Dec 10;62(23):2199-204. doi: 10.1016/j.jacc.2013.08.1623. Epub 2013 Sep 18. J Am Coll Cardiol. 2013. PMID: 24055744
-
Should we recommend oral anticoagulation therapy in patients with atrial fibrillation undergoing coronary artery stenting with a high HAS-BLED bleeding risk score?Circ Cardiovasc Interv. 2012 Aug 1;5(4):459-66. doi: 10.1161/CIRCINTERVENTIONS.112.968792. Epub 2012 Jul 10. Circ Cardiovasc Interv. 2012. PMID: 22787018
-
Diagnostic Accuracy of the HAS-BLED Bleeding Score in VKA- or DOAC-Treated Patients With Atrial Fibrillation: A Systematic Review and Meta-Analysis.Front Cardiovasc Med. 2021 Nov 22;8:757087. doi: 10.3389/fcvm.2021.757087. eCollection 2021. Front Cardiovasc Med. 2021. PMID: 34881309 Free PMC article.
-
Robotics-assisted epicardial left atrial appendage clip exclusion.JTCVS Tech. 2021 Jul 21;9:59-68. doi: 10.1016/j.xjtc.2021.07.009. eCollection 2021 Oct. JTCVS Tech. 2021. PMID: 34647061 Free PMC article.
-
Stroke and bleeding risk in atrial fibrillation.Korean Circ J. 2014 Sep;44(5):281-90. doi: 10.4070/kcj.2014.44.5.281. Korean Circ J. 2014. PMID: 25278980 Free PMC article. Review.
Cited by
-
The Efficacy and Safety of Cilostazol vs. Aspirin for Secondary Stroke Prevention: A Systematic Review and Meta-Analysis.Front Neurol. 2022 Feb 15;13:814654. doi: 10.3389/fneur.2022.814654. eCollection 2022. Front Neurol. 2022. PMID: 35242099 Free PMC article.
-
Assessment of one-year risk of ischemic stroke versus major bleeding in patients with atrial fibrillation.Int J Cardiol Cardiovasc Risk Prev. 2022 Mar 25;13:200129. doi: 10.1016/j.ijcrp.2022.200129. eCollection 2022 Jun. Int J Cardiol Cardiovasc Risk Prev. 2022. PMID: 35403171 Free PMC article.
References
-
- Hu D, Sun Y. Epidemiology, risk factors for stroke, and management of atrial fibrillation in China. J Am Coll Cardiol. 2008;52(10):865–868. - PubMed
-
- Yan L, Fan Z. Progress in the new drugs for treatment of atrial fibrillation. Zhongguo Lin Chuang Yao Li Xue Za Zhi. 2011;1:64–67.
-
- Rahman F, Kwan G F, Benjamin E J. Global epidemiology of atrial fibrillation. Nat Rev Cardiol. 2014;11(11):639–654. - PubMed
-
- Lip G YH, Potpara T, Boriani G, Blomström-Lundqvist C. A tailored treatment strategy: a modern approach for stroke prevention in patients with atrial fibrillation. J Intern Med. 2016;279(05):467–476. - PubMed
-
- Proietti M, Mujovic N, Potpara T S. Optimizing stroke and bleeding risk assessment in patients with atrial fibrillation: a balance of evidence, practicality and precision. Thromb Haemost. 2018;118(12):2014–2017. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
