

The influence of the SARS-CoV-2 pandemic on esophagogastric cancer services: an international survey of esophagogastric surgeons
- PMID: 32500134
- PMCID: PMC7314222
- DOI: 10.1093/dote/doaa054
The influence of the SARS-CoV-2 pandemic on esophagogastric cancer services: an international survey of esophagogastric surgeons
Erratum in
-
Corrigendum to: The influence of the SARS-CoV-2 pandemic on esophagogastric cancer services: an international survey of esophagogastric surgeons.Dis Esophagus. 2021 Aug 10;34(8):doab035. doi: 10.1093/dote/doab035. Dis Esophagus. 2021. PMID: 33963749 Free PMC article. No abstract available.
Abstract
Background: Several guidelines to guide clinical practice among esophagogastric surgeons during the COVID-19 pandemic were produced. However, none provide reflection of current service provision. This international survey aimed to clarify the changes observed in esophageal and gastric cancer management and surgery during the COVID-19 pandemic.
Methods: An online survey covering key areas for esophagogastric cancer services, including staging investigations and oncological and surgical therapy before and during (at two separate time-points-24th March 2020 and 18th April 2020) the COVID-19 pandemic were developed.
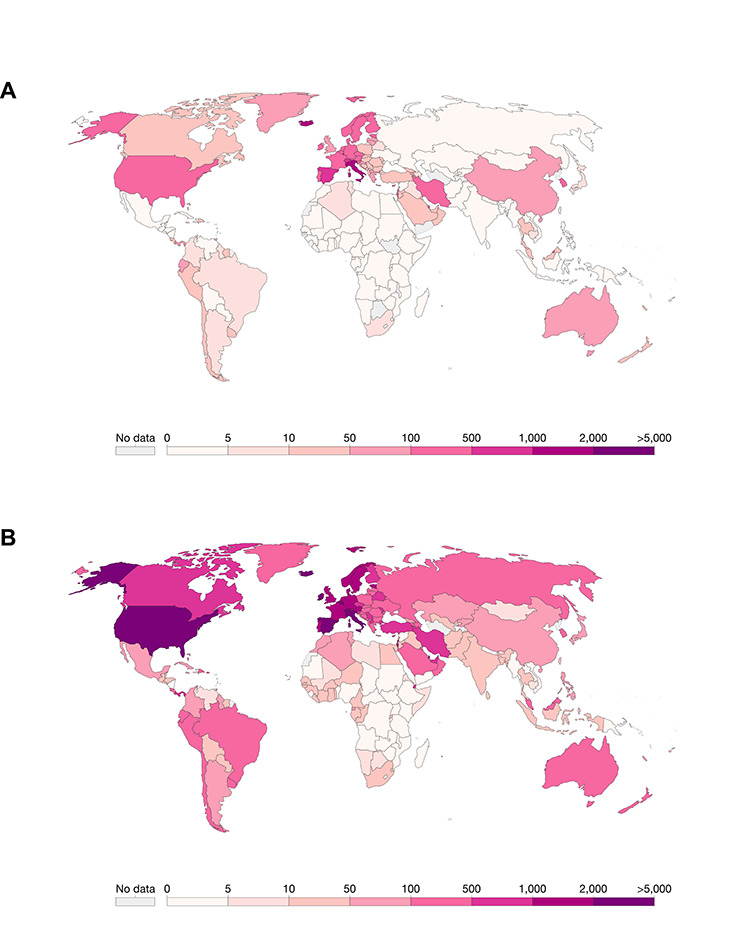
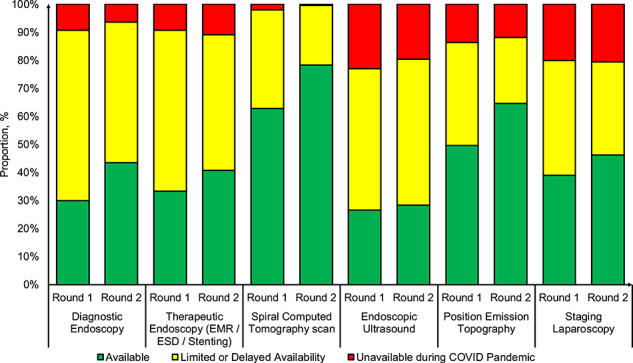
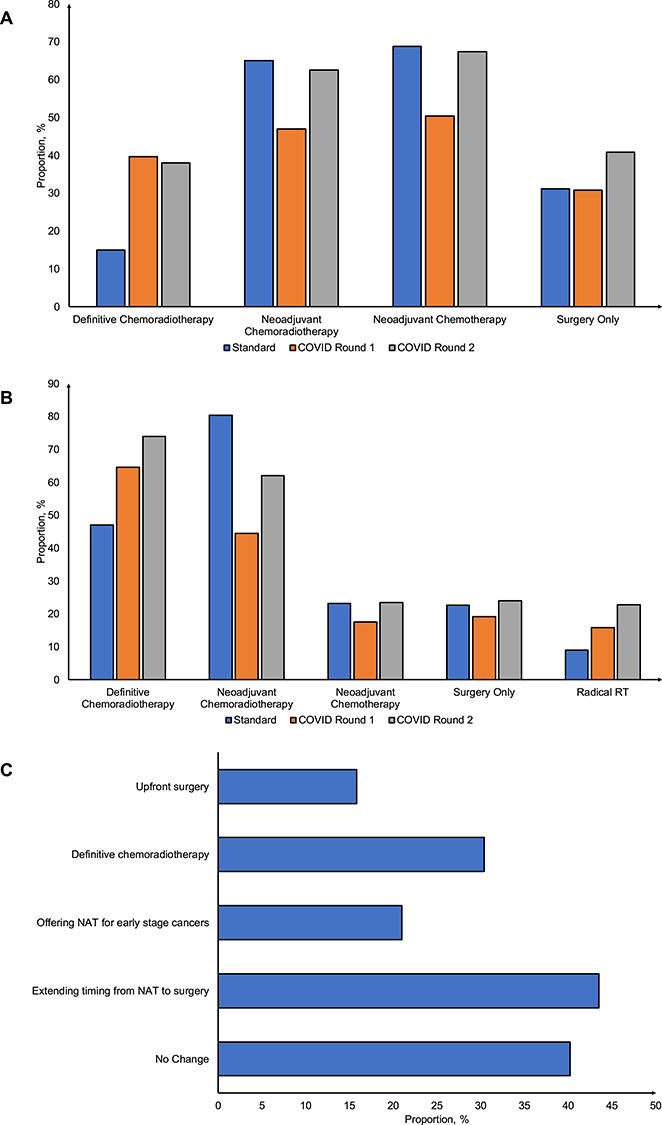
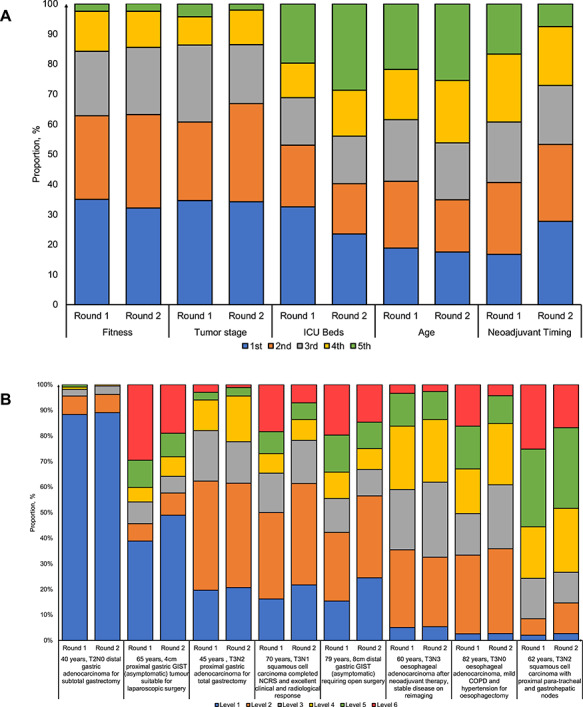
Results: A total of 234 respondents from 225 centers and 49 countries spanning six continents completed the first round of the online survey, of which 79% (n = 184) completed round 2. There was variation in the availability of staging investigations ranging from 26.5% for endoscopic ultrasound to 62.8% for spiral computed tomography scan. Definitive chemoradiotherapy was offered in 14.8% (adenocarcinoma) and 47.0% (squamous cell carcinoma) of respondents and significantly increased by almost three-fold and two-fold, respectively, in both round 1 and 2. There were uncertainty and heterogeneity surrounding prioritization of patients undergoing cancer resections. Of the surgeons symptomatic with COVID-19, only 40.2% (33/82) had routine access to COVID-19 polymerase chain reaction testing for staff. Of those who had testing available (n = 33), only 12.1% (4/33) had tested positive.
Conclusions: These data highlight management challenges and several practice variations in caring for patients with esophagogastric cancers. Therefore, there is a need for clear consistent guidelines to be in place in the event of a further pandemic to ensure a standardized level of oncological care for patients with esophagogastric cancers.
Keywords: COVID-19; SARS-CoV-2; esophageal cancer; esophageal surgery; gastric cancer; pandemic.
© Crown copyright 2020.
Figures
References
-
- World Health Organization Coronavirus Disease 2019 (COVID-19): Situation Report, 2020, 103 [Cited 2 May 2020]Available fromhttps://www.who.int/docs/default-source/coronaviruse/situation-reports/2...
-
- Grasselli G, Pesenti A, Cecconi M. Critical care utilization for the COVID-19 outbreak in Lombardy, Italy: early experience and forecast during an emergency response. JAMA 2020. - PubMed
-
- Pellino G, Spinelli A. How COVID-19 outbreak is impacting colorectal cancer patients in Italy: a long shadow beyond infection. Dis Colon Rectum 2020. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
