

Cardiac cine magnetic resonance fingerprinting for combined ejection fraction, T1 and T2 quantification
- PMID: 32500541
- PMCID: PMC7772953
- DOI: 10.1002/nbm.4323
Cardiac cine magnetic resonance fingerprinting for combined ejection fraction, T1 and T2 quantification
Abstract
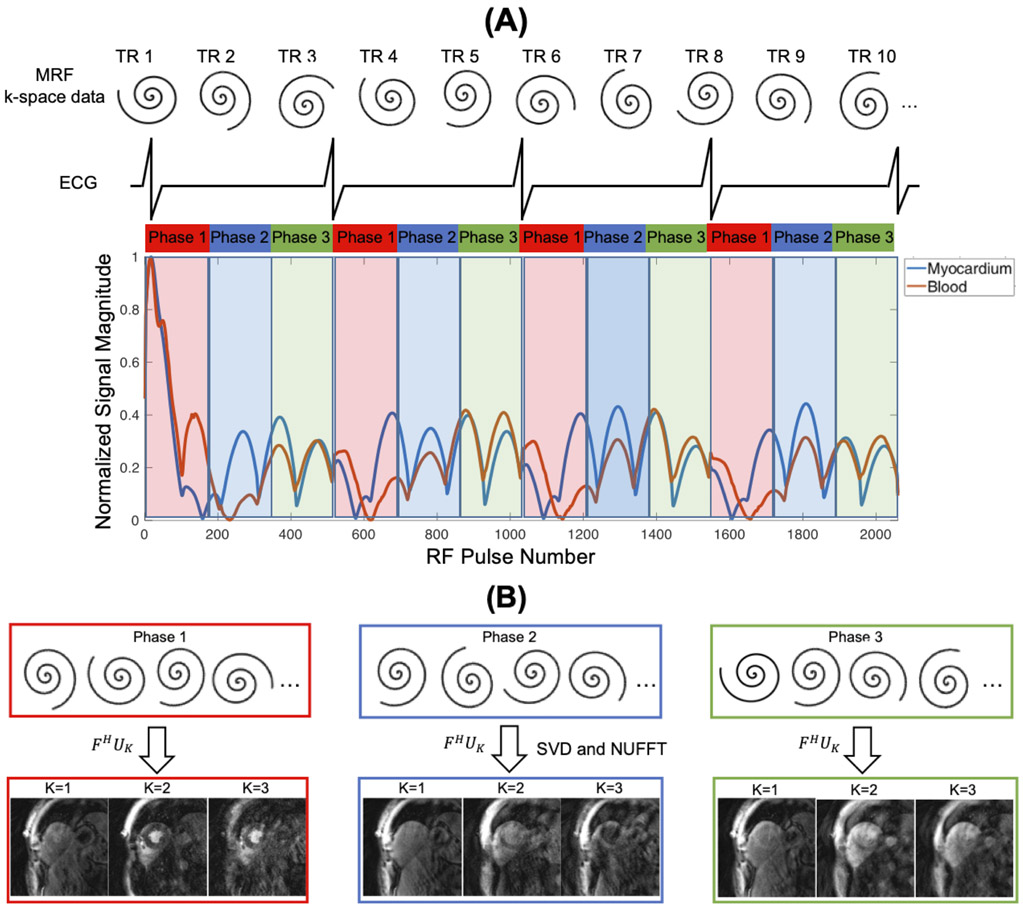
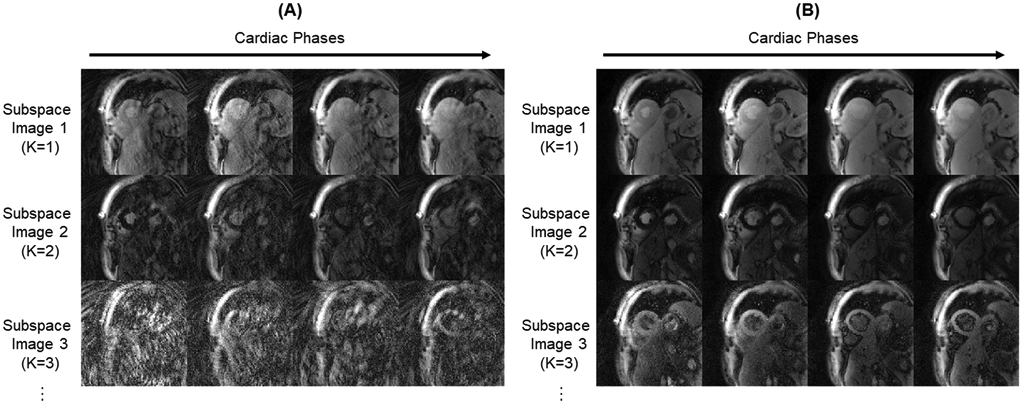
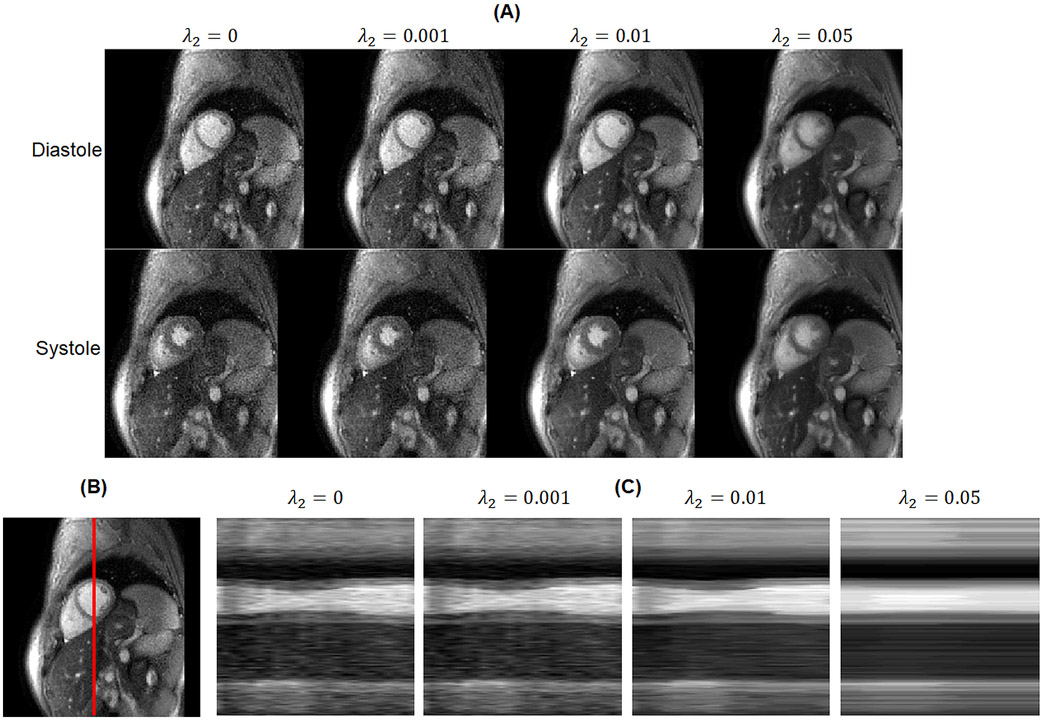
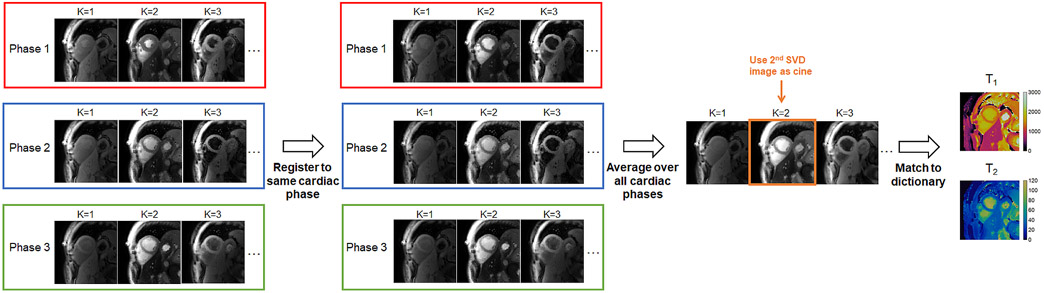
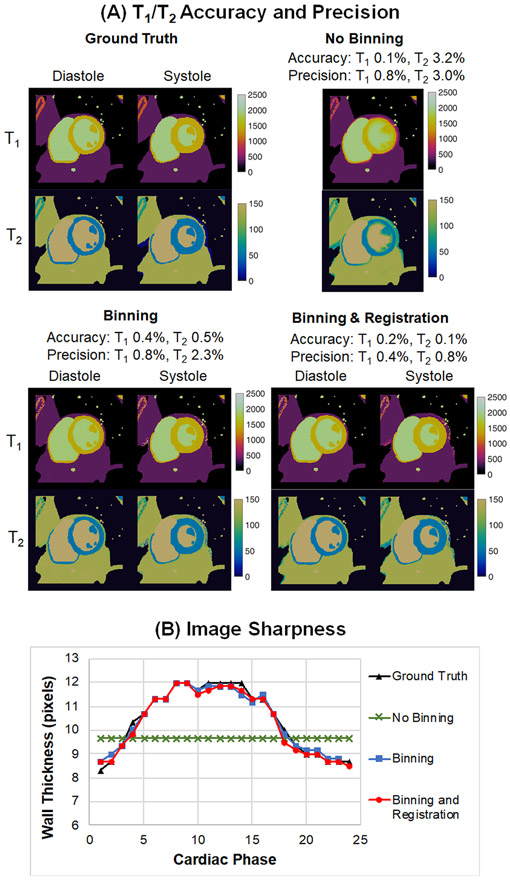
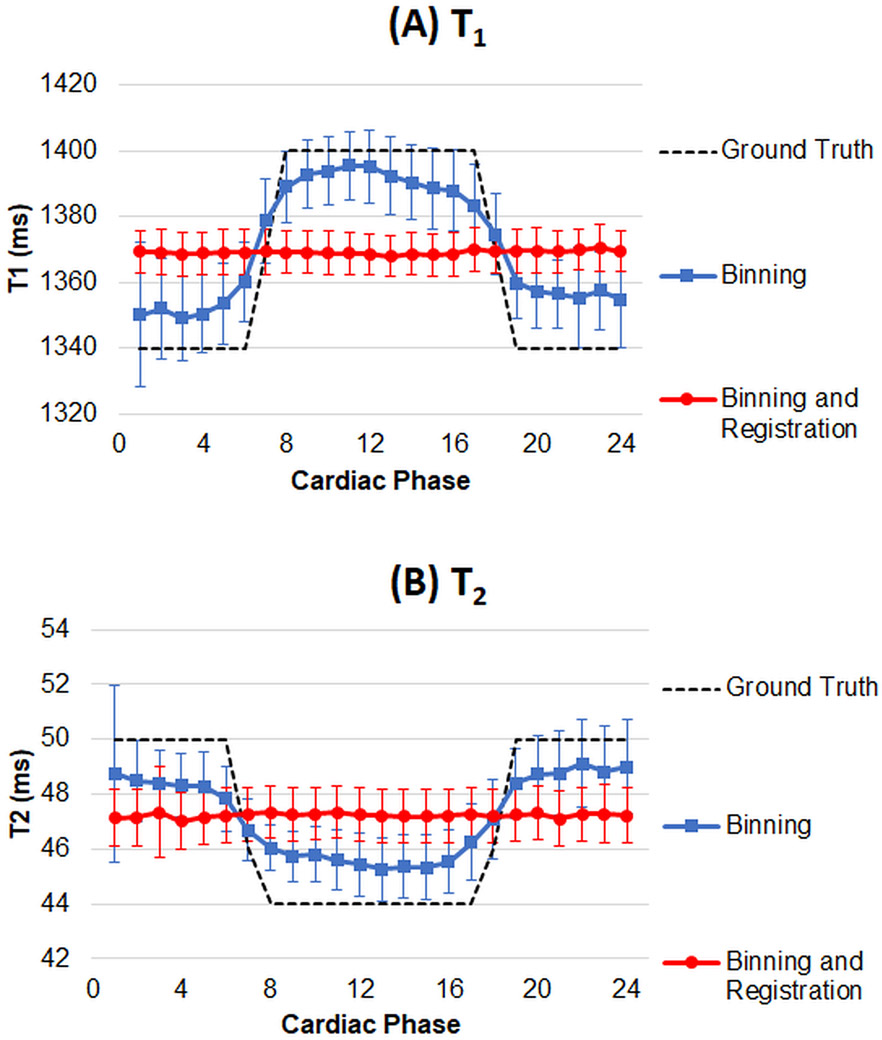
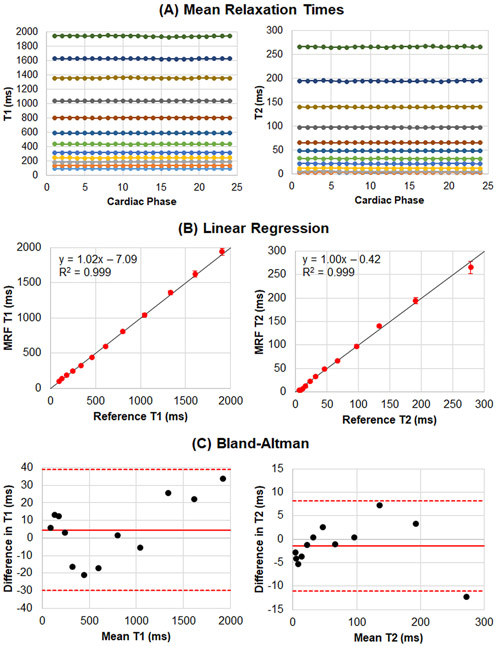
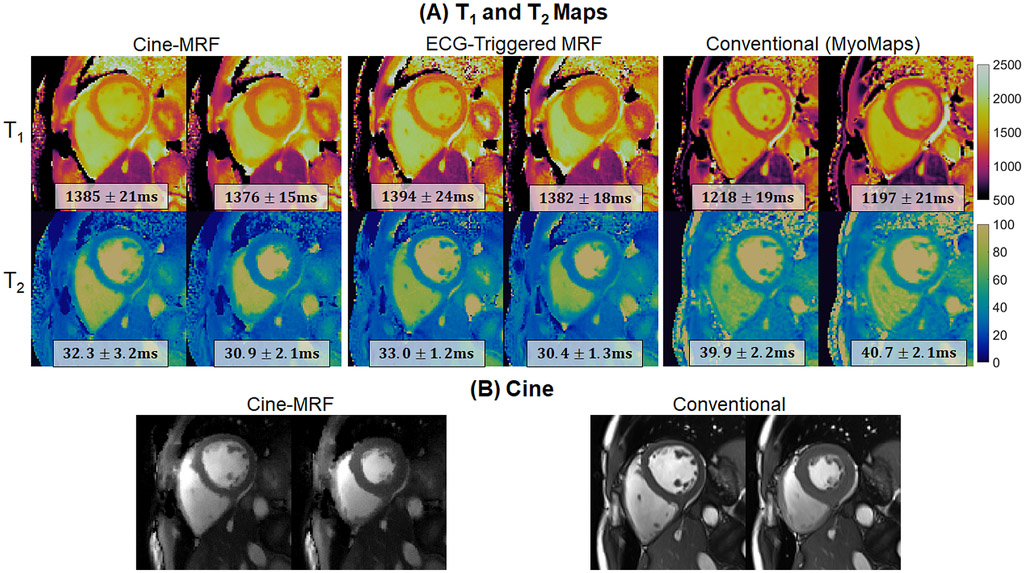
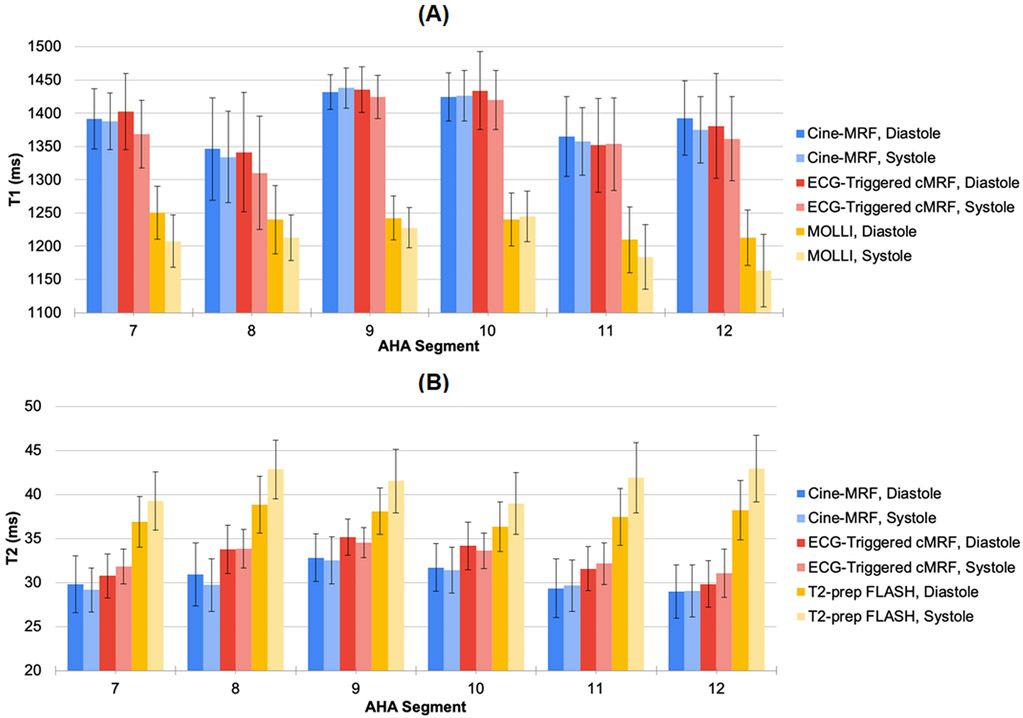
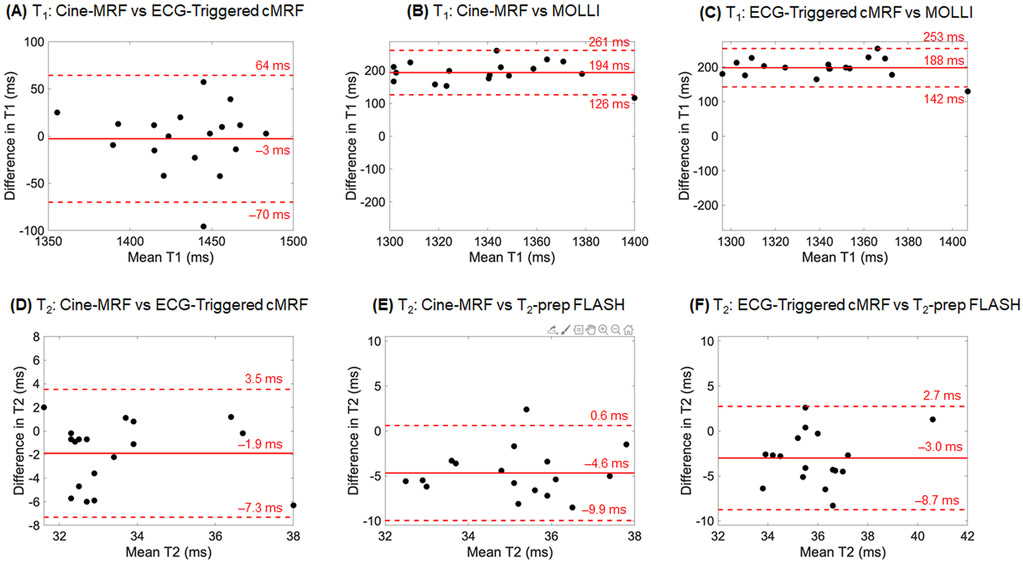
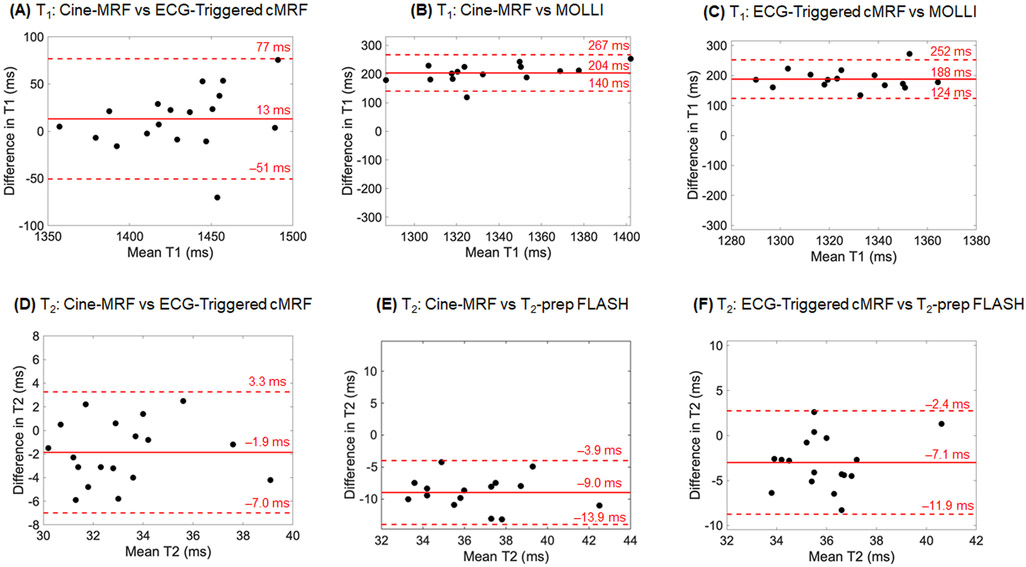
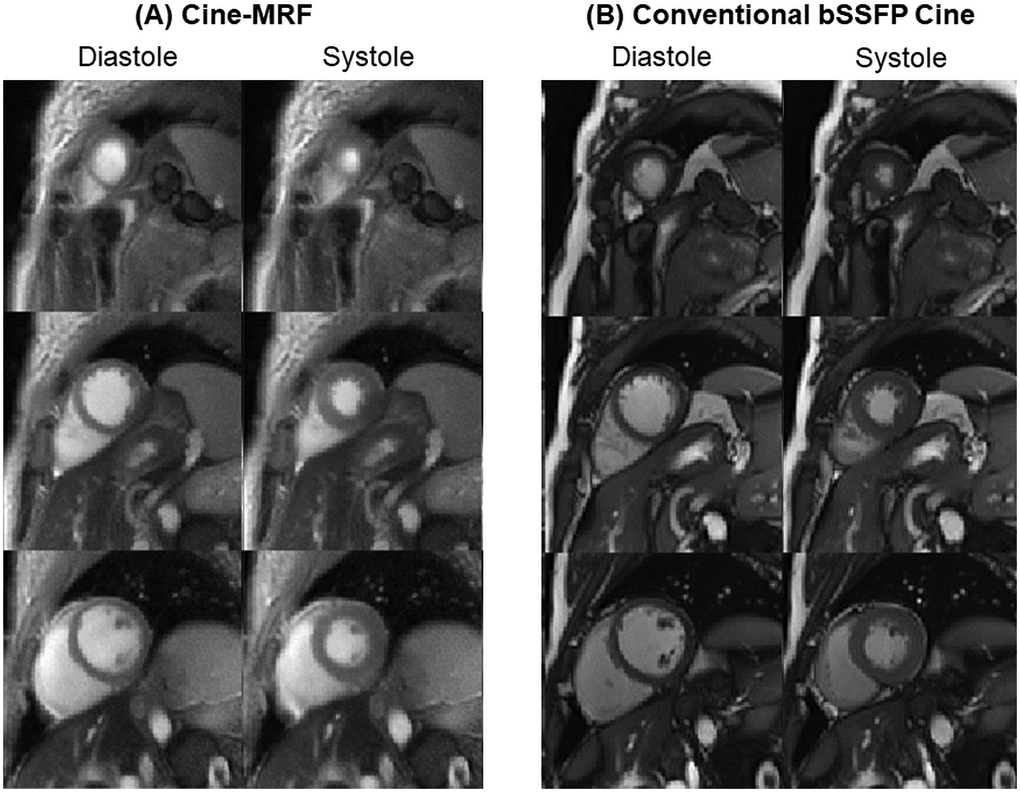
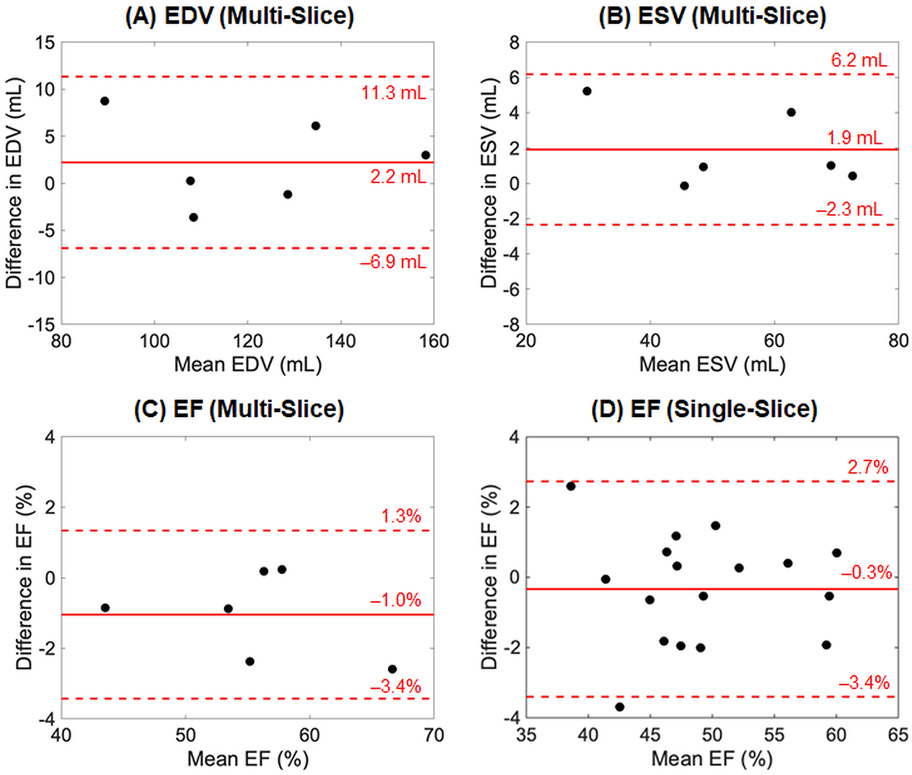
This study introduces a technique called cine magnetic resonance fingerprinting (cine-MRF) for simultaneous T1 , T2 and ejection fraction (EF) quantification. Data acquired with a free-running MRF sequence are retrospectively sorted into different cardiac phases using an external electrocardiogram (ECG) signal. A low-rank reconstruction with a finite difference sparsity constraint along the cardiac motion dimension yields images resolved by cardiac phase. To improve SNR and precision in the parameter maps, these images are nonrigidly registered to the same phase and matched to a dictionary to generate T1 and T2 maps. Cine images for computing left ventricular volumes and EF are also derived from the same data. Cine-MRF was tested in simulations using a numerical relaxation phantom. Phantom and in vivo scans of 19 subjects were performed at 3 T during a 10.9 seconds breath-hold with an in-plane resolution of 1.6 x 1.6 mm2 and 24 cardiac phases. Left ventricular EF values obtained with cine-MRF agreed with the conventional cine images (mean bias -1.0%). Average myocardial T1 times in diastole/systole were 1398/1391 ms with cine-MRF, 1394/1378 ms with ECG-triggered cardiac MRF (cMRF) and 1234/1212 ms with MOLLI; and T2 values were 30.7/30.3 ms with cine-MRF, 32.6/32.9 ms with ECG-triggered cMRF and 37.6/41.0 ms with T2 -prepared FLASH. Cine-MRF and ECG-triggered cMRF relaxation times were in good agreement. Cine-MRF T1 values were significantly longer than MOLLI, and cine-MRF T2 values were significantly shorter than T2 -prepared FLASH. In summary, cine-MRF can potentially streamline cardiac MRI exams by combining left ventricle functional assessment and T1 -T2 mapping into one time-efficient acquisition.
Keywords: cine, ejection fraction, low rank, magnetic resonance fingerprinting, myocardial tissue characterization, T1 mapping, T2 mapping.
© 2020 John Wiley & Sons, Ltd.
Figures
References
-
- Bogaert J, Dymarkowski S, Taylor AM, Muthurangu V. Clinical Cardiac MRI. 2nd ed. Springer-Verlag; Berlin Heidelberg; 2012.
-
- Hinojar R, Nagel E, Puntmann VO. T1 mapping in myocarditis - headway to a new era for cardiovascular magnetic resonance. Expert Rev Cardiovasc Ther. 2015;13(8):871–874. - PubMed
-
- Goldfarb JW, Arnold S, Han J. Recent myocardial infarction: assessment with unenhanced T1-weighted MR imaging. Radiology. 2007;245(1):245–250. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
