

Airway Management in the Operating Room and Interventional Suites in Known or Suspected COVID-19 Adult Patients: A Practical Review
- PMID: 32502132
- PMCID: PMC7288783
- DOI: 10.1213/ANE.0000000000005043
Airway Management in the Operating Room and Interventional Suites in Known or Suspected COVID-19 Adult Patients: A Practical Review
Abstract
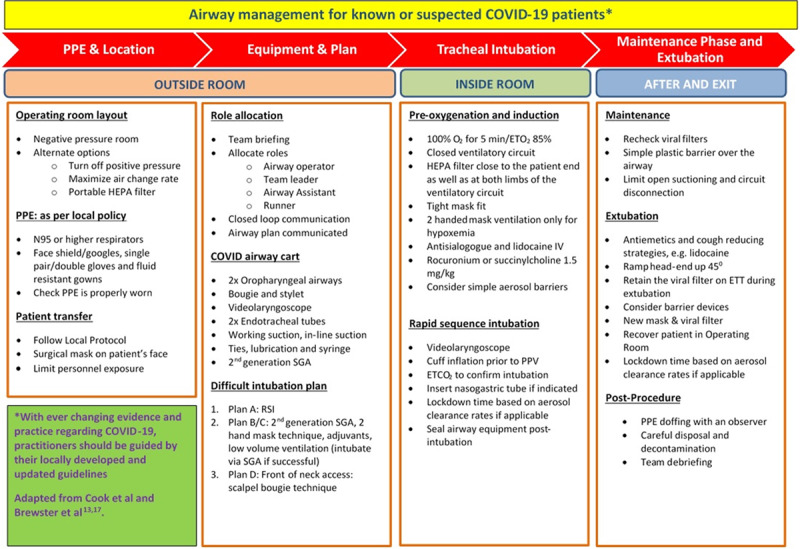
Current evidence suggests that coronavirus disease 2019 (COVID-19) spread occurs via respiratory droplets (particles >5 µm) and possibly through aerosol. The rate of transmission remains high during airway management. This was evident during the 2003 severe acute respiratory syndrome epidemic where those who were involved in tracheal intubation had a higher risk of infection than those who were not involved (odds ratio 6.6). We describe specific airway management principles for patients with known or suspected COVID-19 disease for an array of critical care and procedural settings. We conducted a thorough search of the available literature of airway management of COVID-19 across a variety of international settings. In addition, we have analyzed various medical professional body recommendations for common procedural practices such as interventional cardiology, gastroenterology, and pulmonology. A systematic process that aims to protect the operators involved via appropriate personal protective equipment, avoidance of unnecessary patient contact and minimalization of periprocedural aerosol generation are key components to successful airway management. For operating room cases requiring general anesthesia or complex interventional procedures, tracheal intubation should be the preferred option. For interventional procedures, when tracheal intubation is not indicated, cautious conscious sedation appears to be a reasonable approach. Awake intubation should be avoided unless it is absolutely necessary. Extubation is a high-risk procedure for aerosol and droplet spread and needs thorough planning and preparation. As updates and modifications in the management of COVID-19 are still evolving, local guidelines, appraised at regular intervals, are vital in optimizing clinical management.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Comment in
-
In Response.Anesth Analg. 2021 Mar 1;132(3):e43-e44. doi: 10.1213/ANE.0000000000005338. Anesth Analg. 2021. PMID: 33591101 No abstract available.
References
-
- Paterlini M. On the front lines of coronavirus: the Italian response to COVID-19. BMJ. 2020;368:m1065. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
