

Using machine learning models to predict the initiation of renal replacement therapy among chronic kidney disease patients
- PMID: 32502209
- PMCID: PMC7274378
- DOI: 10.1371/journal.pone.0233976
Using machine learning models to predict the initiation of renal replacement therapy among chronic kidney disease patients
Abstract
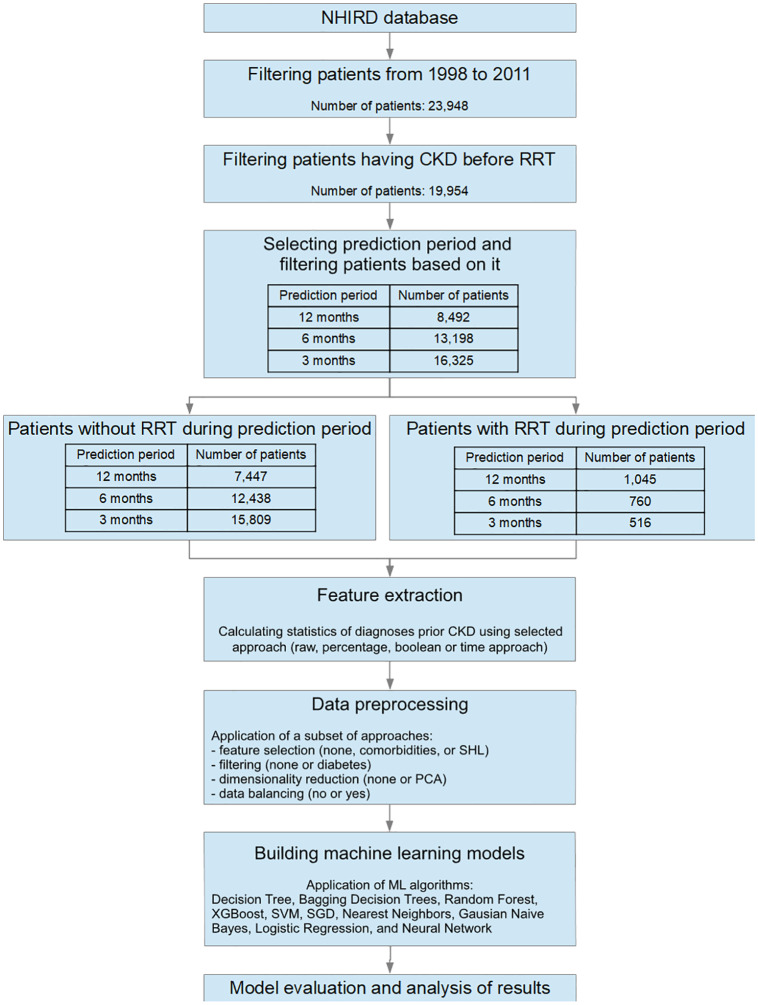
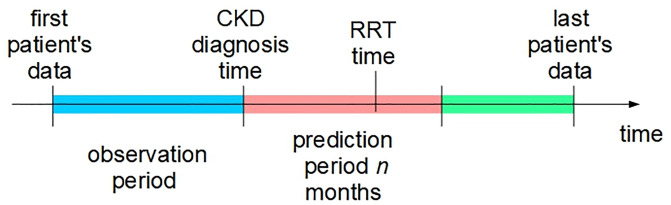
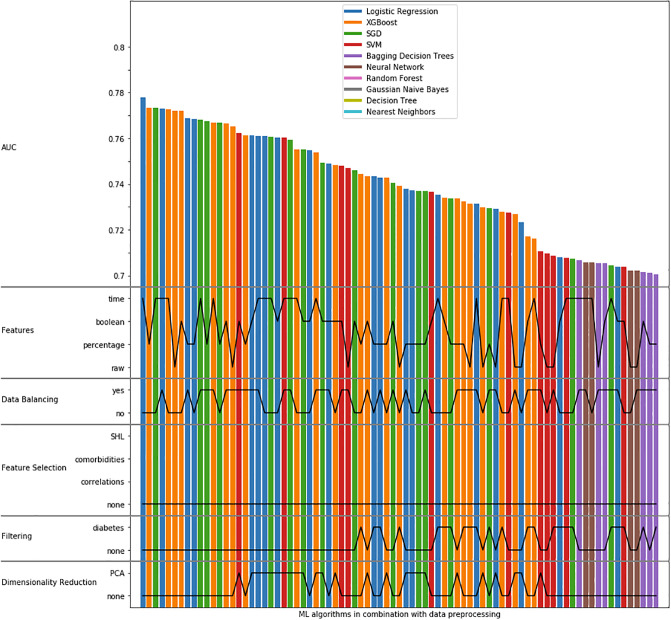
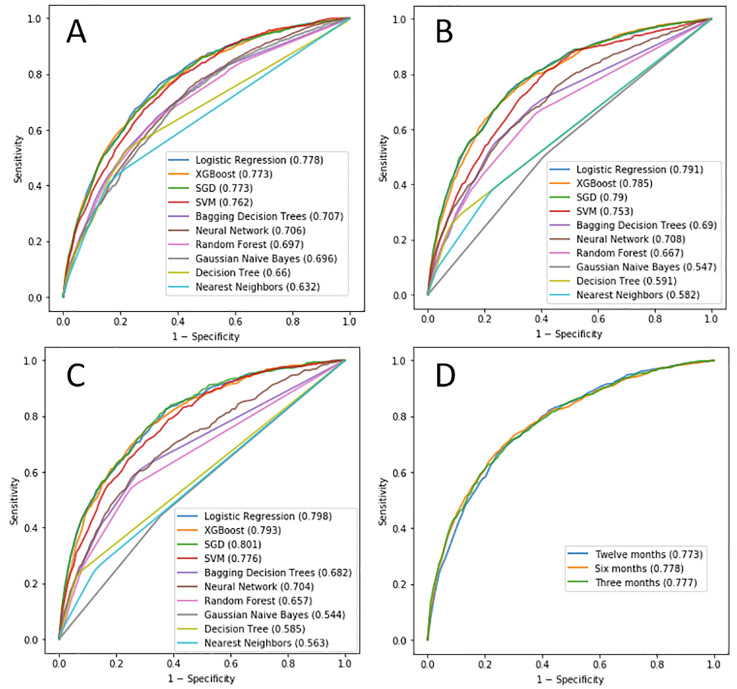
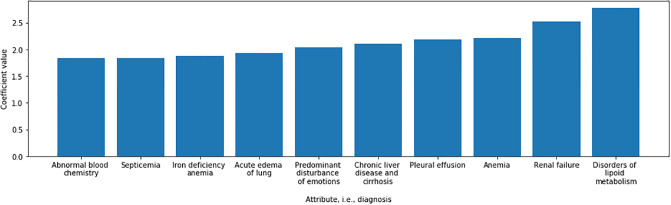
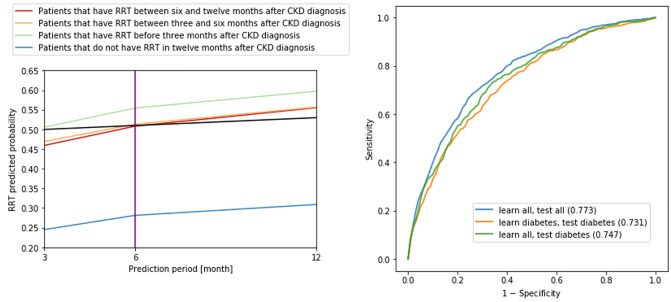
Starting renal replacement therapy (RRT) for patients with chronic kidney disease (CKD) at an optimal time, either with hemodialysis or kidney transplantation, is crucial for patient's well-being and for successful management of the condition. In this paper, we explore the possibilities of creating forecasting models to predict the onset of RRT 3, 6, and 12 months from the time of the patient's first diagnosis with CKD, using only the comorbidities data from National Health Insurance from Taiwan. The goal of this study was to see whether a limited amount of data (including comorbidities but not considering laboratory values which are expensive to obtain in low- and medium-income countries) can provide a good basis for such predictive models. On the other hand, in developed countries, such models could allow policy-makers better planning and allocation of resources for treatment. Using data from 8,492 patients, we obtained the area under the receiver operating characteristic curve (AUC) of 0.773 for predicting RRT within 12 months from the time of CKD diagnosis. The results also show that there is no additional advantage in focusing only on patients with diabetes in terms of prediction performance. Although these results are not as such suitable for adoption into clinical practice, the study provides a strong basis and a variety of approaches for future studies of forecasting models in healthcare.
Conflict of interest statement
The authors acknowledge the financial support from the Slovenian Research Agency (research core funding No. P2-0209). This work is part of the CrowdHEALTH project that has received funding from the European Union’s Horizon 2020 research and innovation program under grant agreement no. 727560 (JSI) and Ministry of Science and Technology under project no. 106-3805-018-110 (TMU). We gratefully acknowledge the support of NVIDIA Corporation with the donation of the Titan V GPU used for this research. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
