

Effects of non-pharmaceutical interventions on COVID-19 cases, deaths, and demand for hospital services in the UK: a modelling study
- PMID: 32502389
- PMCID: PMC7266572
- DOI: 10.1016/S2468-2667(20)30133-X
Effects of non-pharmaceutical interventions on COVID-19 cases, deaths, and demand for hospital services in the UK: a modelling study
Abstract
Background: Non-pharmaceutical interventions have been implemented to reduce transmission of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in the UK. Projecting the size of an unmitigated epidemic and the potential effect of different control measures has been crucial to support evidence-based policy making during the early stages of the epidemic. This study assesses the potential impact of different control measures for mitigating the burden of COVID-19 in the UK.
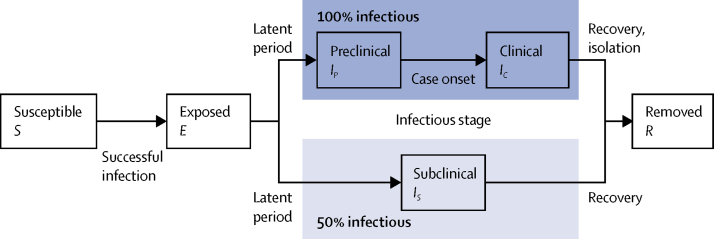
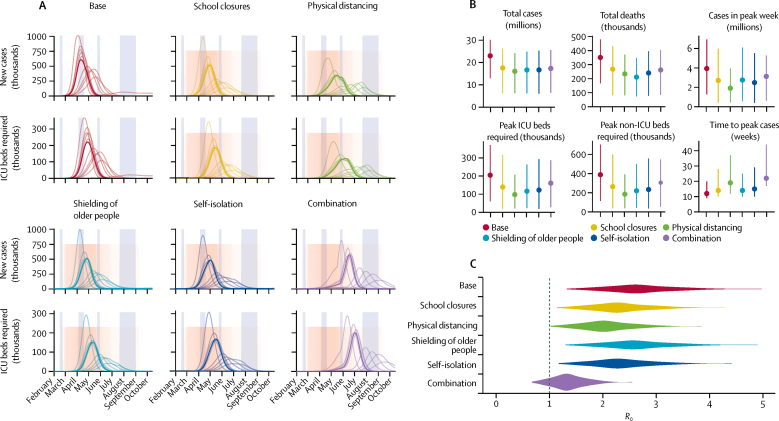
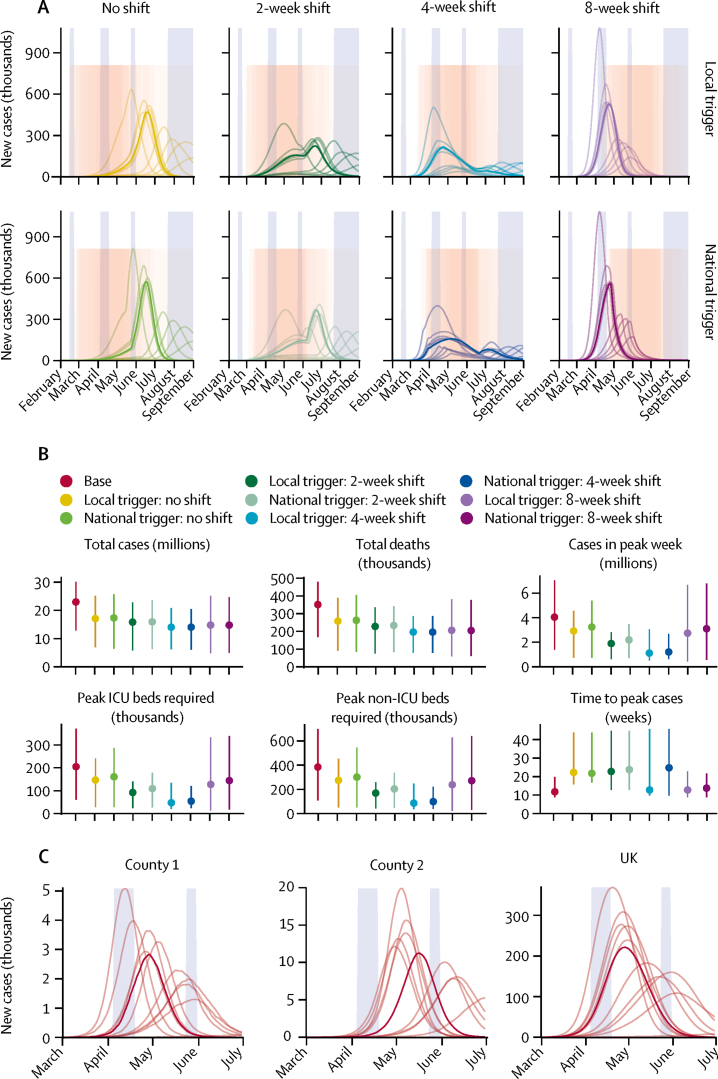
Methods: We used a stochastic age-structured transmission model to explore a range of intervention scenarios, tracking 66·4 million people aggregated to 186 county-level administrative units in England, Wales, Scotland, and Northern Ireland. The four base interventions modelled were school closures, physical distancing, shielding of people aged 70 years or older, and self-isolation of symptomatic cases. We also modelled the combination of these interventions, as well as a programme of intensive interventions with phased lockdown-type restrictions that substantially limited contacts outside of the home for repeated periods. We simulated different triggers for the introduction of interventions, and estimated the impact of varying adherence to interventions across counties. For each scenario, we projected estimated new cases over time, patients requiring inpatient and critical care (ie, admission to the intensive care units [ICU]) treatment, and deaths, and compared the effect of each intervention on the basic reproduction number, R0.
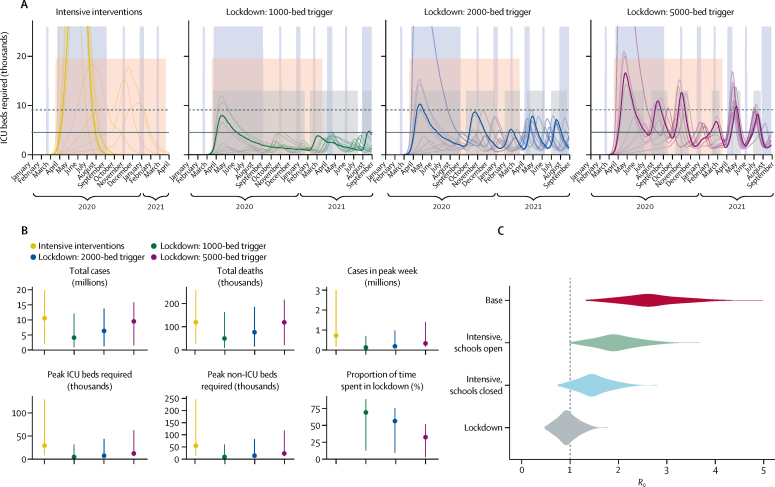
Findings: We projected a median unmitigated burden of 23 million (95% prediction interval 13-30) clinical cases and 350 000 deaths (170 000-480 000) due to COVID-19 in the UK by December, 2021. We found that the four base interventions were each likely to decrease R0, but not sufficiently to prevent ICU demand from exceeding health service capacity. The combined intervention was more effective at reducing R0, but only lockdown periods were sufficient to bring R0 near or below 1; the most stringent lockdown scenario resulted in a projected 120 000 cases (46 000-700 000) and 50 000 deaths (9300-160 000). Intensive interventions with lockdown periods would need to be in place for a large proportion of the coming year to prevent health-care demand exceeding availability.
Interpretation: The characteristics of SARS-CoV-2 mean that extreme measures are probably required to bring the epidemic under control and to prevent very large numbers of deaths and an excess of demand on hospital beds, especially those in ICUs.
Funding: Medical Research Council.
Copyright © 2020 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Unlocking UK COVID-19 policy.Lancet Public Health. 2020 Jul;5(7):e362-e363. doi: 10.1016/S2468-2667(20)30135-3. Epub 2020 Jun 2. Lancet Public Health. 2020. PMID: 32502388 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
