

Quality of life in patients with cervical cancer after open versus minimally invasive radical hysterectomy (LACC): a secondary outcome of a multicentre, randomised, open-label, phase 3, non-inferiority trial
- PMID: 32502445
- PMCID: PMC9762514
- DOI: 10.1016/S1470-2045(20)30081-4
Quality of life in patients with cervical cancer after open versus minimally invasive radical hysterectomy (LACC): a secondary outcome of a multicentre, randomised, open-label, phase 3, non-inferiority trial
Erratum in
-
Correction to Lancet Oncol 2020; 21: 851-60.Lancet Oncol. 2020 Jul;21(7):e341. doi: 10.1016/S1470-2045(20)30347-8. Lancet Oncol. 2020. PMID: 32615114 No abstract available.
Abstract
Background: In the phase 3 LACC trial and a subsequent population-level review, minimally invasive radical hysterectomy was shown to be associated with worse disease-free survival and higher recurrence rates than was open radical hysterectomy in patients with early stage cervical cancer. Here, we report the results of a secondary endpoint, quality of life, of the LACC trial.
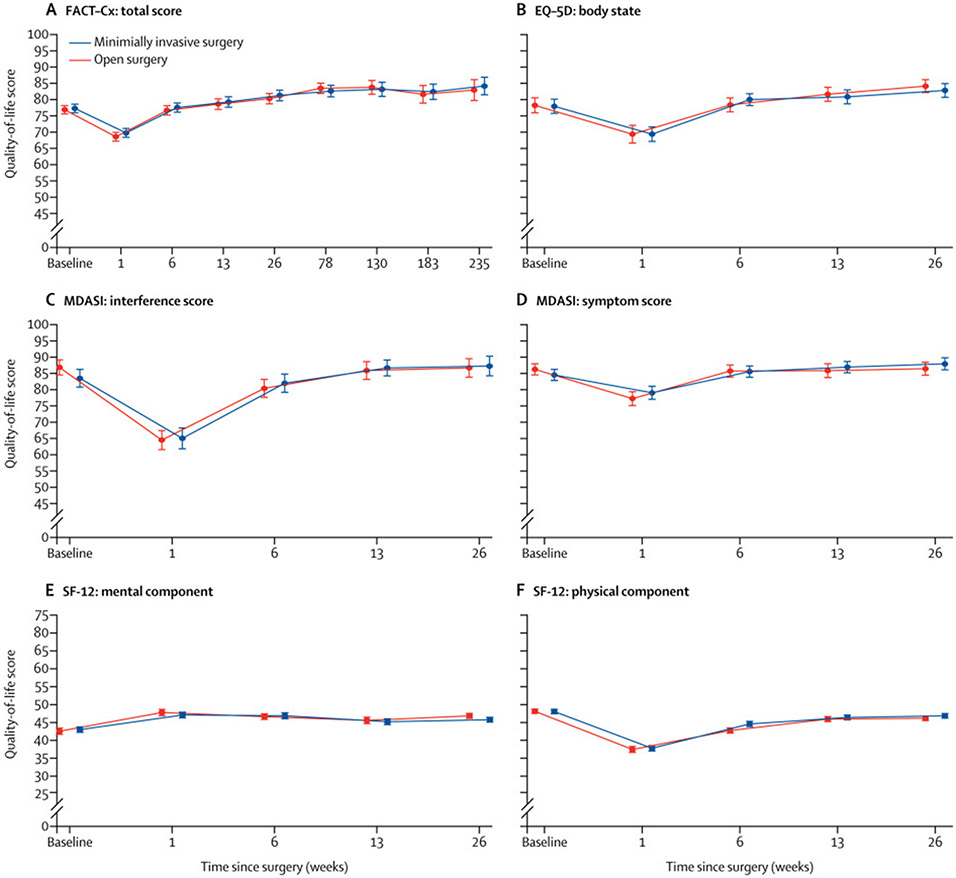
Methods: The LACC trial was a randomised, open-label, phase 3, non-inferiority trial done in 33 centres worldwide. Eligible participants were women aged 18 years or older with International Federation of Gynaecology and Obstetrics (FIGO) stage IA1 with lymphovascular space invasion, IA2, or IB1 adenocarcinoma, squamous cell carcinoma, or adenosquamous carcinoma of the cervix, with an Eastern Cooperative Oncology Group performance status of 0 or 1, who were scheduled to have a type 2 or 3 radical hysterectomy. Participants were randomly assigned (1:1) to receive open or minimally invasive radical hysterectomy. Randomisation was done centrally using a computerised minimisation program, stratified by centre, disease stage according to FIGO guidelines, and age. Neither participants nor investigators were masked to treatment allocation. The primary endpoint of the LACC trial was disease-free survival at 4·5 years, and quality of life was a secondary endpoint. Eligible patients completed validated quality-of-life and symptom assessments (12-item Short Form Health Survey [SF-12], Functional Assessment of Cancer Therapy-Cervical [FACT-Cx], EuroQoL-5D [EQ-5D], and MD Anderson Symptom Inventory [MDASI]) before surgery and at 1 and 6 weeks and 3 and 6 months after surgery (FACT-Cx was also completed at additional timepoints up to 54 months after surgery). Differences in quality of life over time between treatment groups were assessed in the modified intention-to-treat population, which included all patients who had surgery and completed at least one baseline (pretreatment) and one follow-up (at any timepoint after surgery) questionnaire, using generalised estimating equations. The LACC trial is registered with ClinicalTrials.gov, NCT00614211.
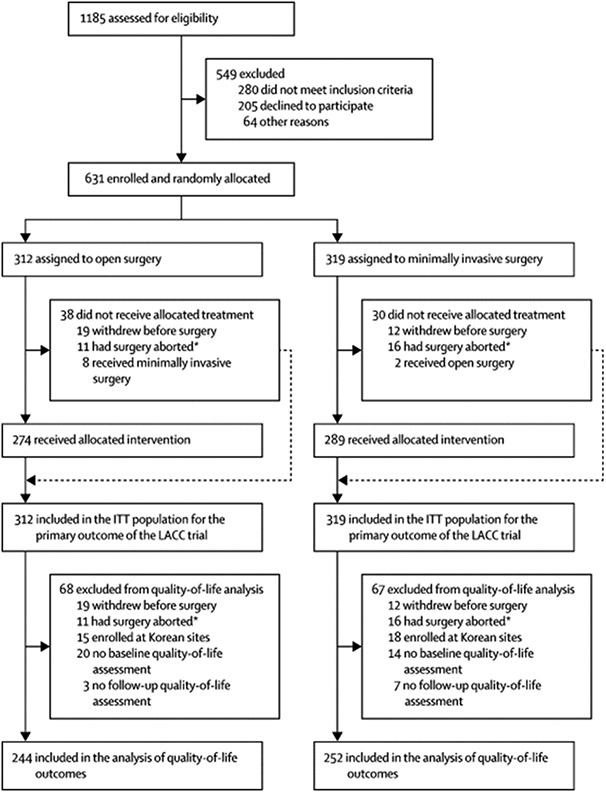
Findings: Between Jan 31, 2008, and June 22, 2017, 631 patients were enrolled; 312 assigned to the open surgery group and 319 assigned to the minimally invasive surgery group. 496 (79%) of 631 patients had surgery completed at least one baseline and one follow-up quality-of-life survey and were included in the modified intention-to-treat analysis (244 [78%] of 312 patients in the open surgery group and 252 [79%] of 319 participants in the minimally invasive surgery group). Median follow-up was 3·0 years (IQR 1·7-4·5). At baseline, no differences in the mean FACT-Cx total score were identified between the open surgery (129·3 [SD 18·8]) and minimally invasive surgery groups (129·8 [19·8]). No differences in mean FACT-Cx total scores were identified between the groups 6 weeks after surgery (128·7 [SD 19·9] in the open surgery group vs 130·0 [19·8] in the minimally invasive surgery group) or 3 months after surgery (132·0 [21·7] vs 133·0 [22·1]).
Interpretation: Since recurrence rates are higher and disease-free survival is lower for minimally invasive radical hysterectomy than for open surgery, and postoperative quality of life is similar between the treatment groups, gynaecological oncologists should recommend open radical hysterectomy for patients with early stage cervical cancer.
Funding: MD Anderson Cancer Center and Medtronic.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of Interests
MF reports grants and personal fees from Novadaq/Stryker, grants from Navidea, personal fees from Johnson and Johnson, personal fees from Genetech, grants from Astra Zeneca, outside the submitted workRLC reports grants from NIH, grants from Gateway Foundation, grants from V Founation, during the conduct of the study; grants and personal fees from AstraZeneca, grants from Merck, personal fees from Tesaro, personal fees from Medivation, grants and personal fees from Clovis, personal fees from Gamamab, grants and personal fees from Genmab, grants and personal fees from Roche/Genentech, grants and personal fees from Janssen, personal fees from Agenus, personal fees from Regeneron, personal fees from OncoQuest, outside the submitted work.
AO reports other from CEO of SurgicalPerformance, a surgical audit software, grants from AO received travel grants from the O.R. Company, non-financial support from AO is a consultant for Covidien, NSW, Australia, outside the submitted work; .
The other authors declare no conflict of interest.
Figures
Comment in
-
Minimally invasive surgery and quality of life in cervical cancer.Lancet Oncol. 2020 Jun;21(6):746-748. doi: 10.1016/S1470-2045(20)30161-3. Lancet Oncol. 2020. PMID: 32502439 No abstract available.
References
-
- Sert BM, Boggess JF, Ahmad S, et al. Robot-assisted versus open radical hysterectomy: A multi-institutional experience for early-stage cervical cancer. Eur J Surg Oncol 2016; 42: 513–22. - PubMed
-
- Nam JH, Park JY, Kim DY, Kim JH, Kim YM, Kim YT. Laparoscopic versus open radical hysterectomy in early-stage cervical cancer: long-term survival outcomes in a matched cohort study. Ann Oncol 2012; 23: 903–11. - PubMed
-
- Corrado G, Vizza E, Legge F, et al. Comparison of Different Surgical Approaches for Stage IB1 Cervical Cancer Patients: A Multi-institution Study and a Review of the Literature. Int J Gynecol Cancer 2018; 28: 1020–8. - PubMed
-
- Ramirez PT, Frumovitz M, Pareja R, et al. Minimally Invasive versus Abdominal Radical Hysterectomy for Cervical Cancer. N Engl J Med 2018; 379: 1895–904. - PubMed
