

Randomized Trial of General Strength and Conditioning Versus Motor Control and Manual Therapy for Chronic Low Back Pain on Physical and Self-Report Outcomes
- PMID: 32503243
- PMCID: PMC7355598
- DOI: 10.3390/jcm9061726
Randomized Trial of General Strength and Conditioning Versus Motor Control and Manual Therapy for Chronic Low Back Pain on Physical and Self-Report Outcomes
Abstract
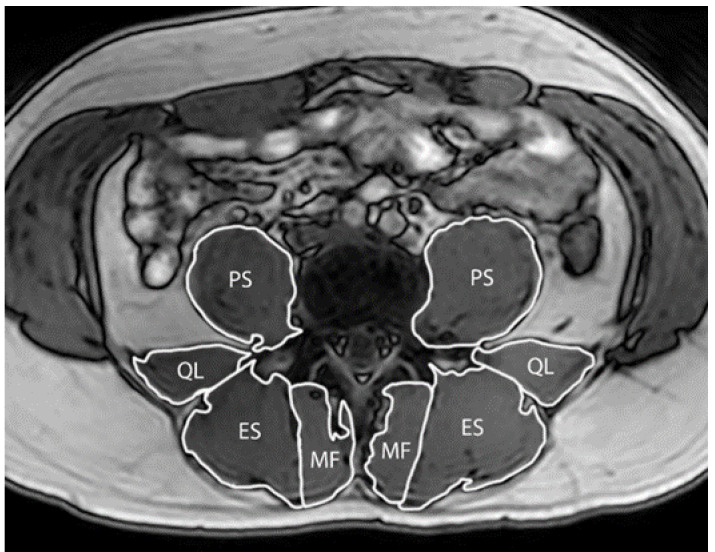
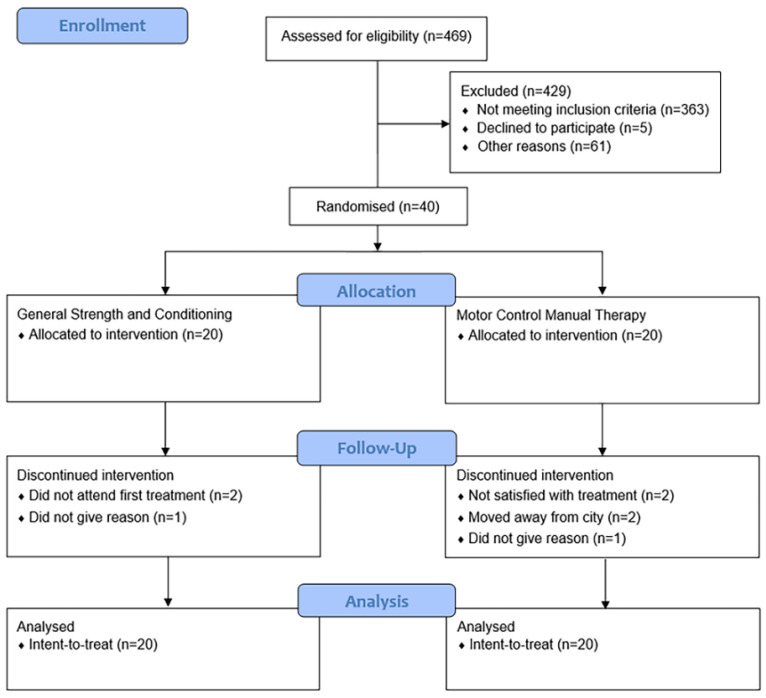
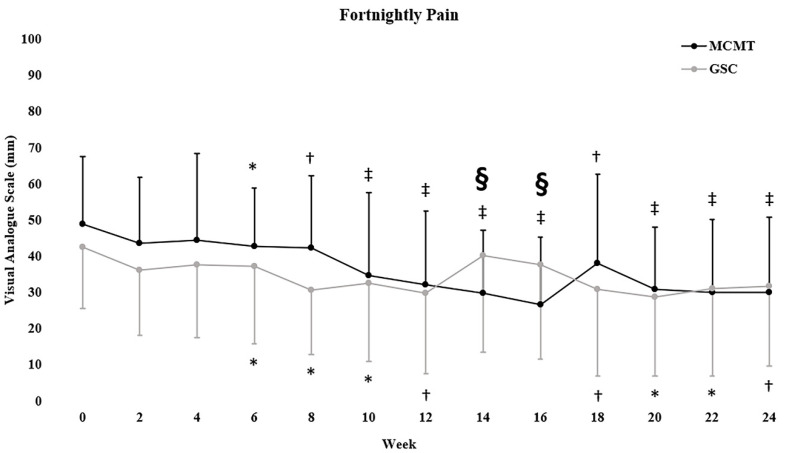
Exercise and spinal manipulative therapy are commonly used for the treatment of chronic low back pain (CLBP) in Australia. Reduction in pain intensity is a common outcome; however, it is only one measure of intervention efficacy in clinical practice. Therefore, we evaluated the effectiveness of two common clinical interventions on physical and self-report measures in CLBP. Participants were randomized to a 6‑month intervention of general strength and conditioning (GSC; n = 20; up to 52 sessions) or motor control exercise plus manual therapy (MCMT; n =20; up to 12 sessions). Pain intensity was measured at baseline and fortnightly throughout the intervention. Trunk extension and flexion endurance, leg muscle strength and endurance, paraspinal muscle volume, cardio‑respiratory fitness and self-report measures of kinesiophobia, disability and quality of life were assessed at baseline and 3- and 6-month follow-up. Pain intensity differed favoring MCMT between-groups at week 14 and 16 of treatment (both, p = 0.003), but not at 6-month follow‑up. Both GSC (mean change (95%CI): -10.7 (-18.7, -2.8) mm; p = 0.008) and MCMT (-19.2 (-28.1, -10.3) mm; p < 0.001) had within-group reductions in pain intensity at six months, but did not achieve clinically meaningful thresholds (20mm) within- or between‑group. At 6-month follow-up, GSC increased trunk extension (mean difference (95% CI): 81.8 (34.8, 128.8) s; p = 0.004) and flexion endurance (51.5 (20.5, 82.6) s; p = 0.004), as well as leg muscle strength (24.7 (3.4, 46.0) kg; p = 0.001) and endurance (9.1 (1.7, 16.4) reps; p = 0.015) compared to MCMT. GSC reduced disability (-5.7 (‑11.2, -0.2) pts; p = 0.041) and kinesiophobia (-6.6 (-9.9, -3.2) pts; p < 0.001) compared to MCMT at 6‑month follow-up. Multifidus volume increased within-group for GSC (p = 0.003), but not MCMT or between-groups. No other between-group changes were observed at six months. Overall, GSC improved trunk endurance, leg muscle strength and endurance, self-report disability and kinesiophobia compared to MCMT at six months. These results show that GSC may provide a more diverse range of treatment effects compared to MCMT.
Keywords: exercise; physical therapy; physiotherapy; rehabilitation; spine.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Vos T., Flaxman A.D., Naghavi M., Lozano R., Michaud C., Ezzati M., Shibuya K., Salomon J.A., Abdalla S., Aboyans V., et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: A systematic analysis for the global burden of disease study 2010. Lancet. 2012;380:2163–2196. doi: 10.1016/S0140-6736(12)61729-2. - DOI - PMC - PubMed
-
- Murray C.J., Vos T., Lozano R., Naghavi M., Flaxman A.D., Michaud C., Ezzati M., Shibuya K., Salomon J.A., Abdalla S., et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2013;380:2197–2223. doi: 10.1016/S0140-6736(12)61689-4. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
