

A modified surgical technique of shortening renal ischemia time in left renal cancer patients with Mayo level II-IV tumor thrombus
- PMID: 32503500
- PMCID: PMC7275451
- DOI: 10.1186/s12893-020-00769-w
A modified surgical technique of shortening renal ischemia time in left renal cancer patients with Mayo level II-IV tumor thrombus
Abstract
Background: To explore the safety and effectiveness of a modified surgical technique which could shorten the time of renal ischemia in left renal cancer and Mayo level II to IV inferior vena cava (IVC) tumor thrombus.
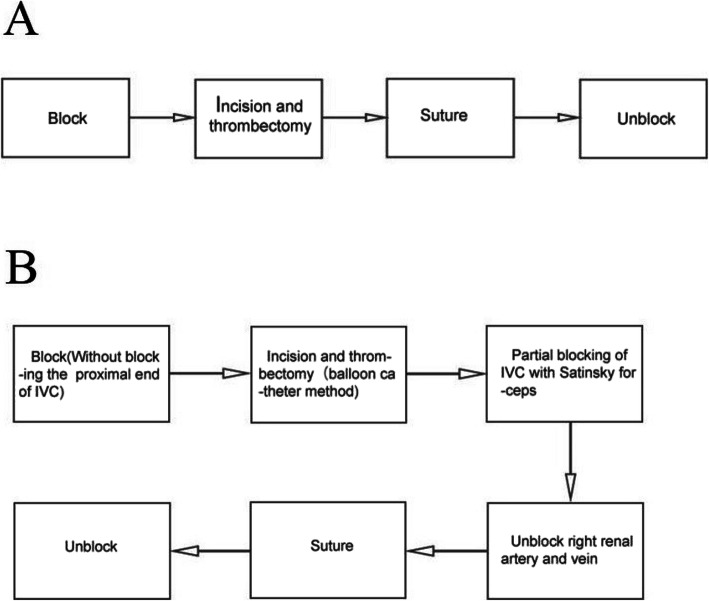
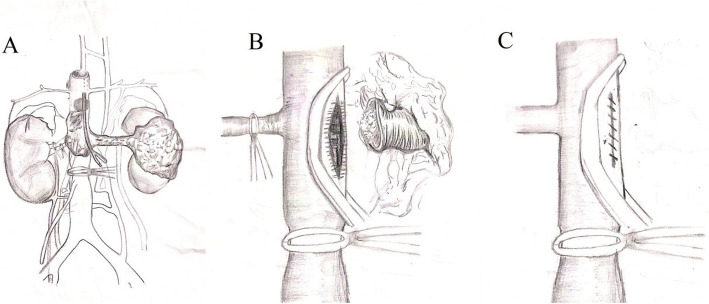
Method: We retrospectively analyzed the clinical data of 14 cases with left renal cell carcinoma (RCC) and Mayo level II to IV IVC tumor thrombus from February 2015 to July 2019. Preoperative imaging showed that there was no obvious sign of tumor thrombus invading the blood vessel wall. During the surgery, after the right renal artery, the right renal vein and the distal end of IVC were blocked, the balloon catheter was used and the tumor thrombus was removed completely from the IVC. The incision of IVC was closed by Satinsky clamp to make IVC partially blocked. Then the right renal artery and right renal vein were released. The incision of IVC was sutured continuously. At last, the Satinsky clamp and the blocking band at the distal end of the IVC were released.
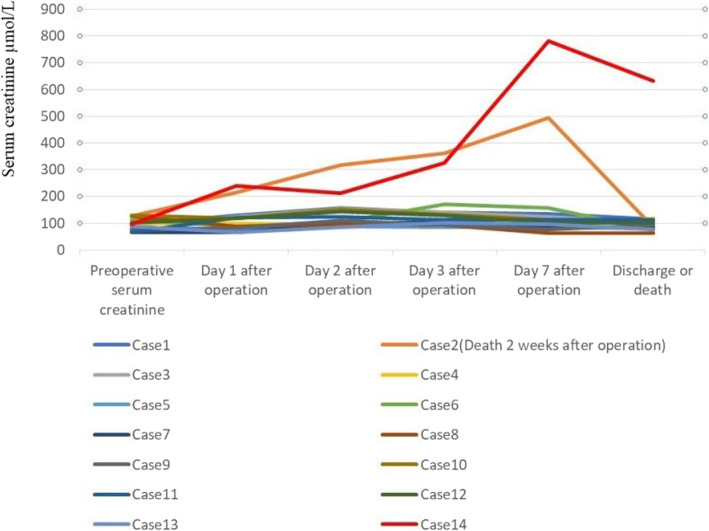
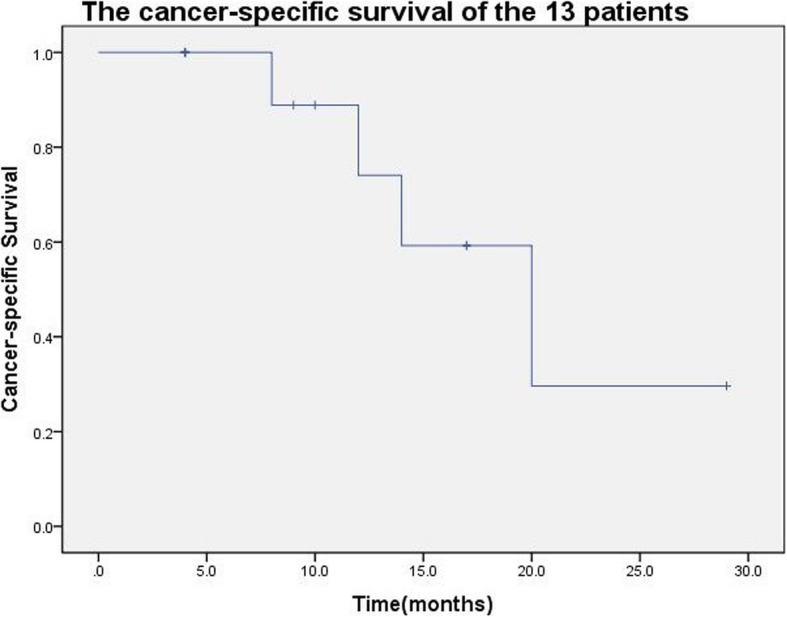
Result: There were 8 cases (57.1%) of Mayo level II, 3 cases (21.4%) of Mayo level III and 3 cases (21.4%) of Mayo level IV. The operation was successfully completed in all 14 patients. There were 2 cases (14.3%) operated by complete laparoscopic approach, 8 cases (57.1%) by open approach, and 4 patients (28.6%) by laparoscopic conversion to open approach. The occlusion time of right renal artery and vein (renal ischemia time) was 3 to 15 min, with an average of (6.8 ± 3.2) minutes. The mean time of IVC occlusion was (19.4 ± 4.9) min. Preoperative creatinine was 66 to 130 μmol/L, with an average of (96.6 ± 21.2) μmol/L. One week after operation, serum creatinine was 64 to 632 μmol/L, with an average of (132.4 ± 144.9) μmol/L. Among the 14 cases, 5 (42.9%) had early postoperative complications. Besides one of the 14 patients died in perioperative period, the median follow-up of other 13 cases was 10 months (range: 4-29 months). The 5 (35.7%) of the 14 cases were died of disease.
Conclusion: This modified procedure was relatively safe and effective in shortening the time of renal ischemia in left RCC patients with Mayo II to IV IVC tumor thrombus.
Keywords: Inferior vena cava; Left side; Renal cancer; Renal ischemia; Tumor thrombus.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
