

Influence of quality of intensive care on quality of life/return to work in survivors of the acute respiratory distress syndrome: prospective observational patient cohort study (DACAPO)
- PMID: 32503583
- PMCID: PMC7275400
- DOI: 10.1186/s12889-020-08943-8
Influence of quality of intensive care on quality of life/return to work in survivors of the acute respiratory distress syndrome: prospective observational patient cohort study (DACAPO)
Abstract
Background: Significant long-term reduction in health-related quality of life (HRQoL) is often observed in survivors of the acute respiratory distress syndrome (ARDS), and return to work (RtW) is limited. There is a paucity of data regarding the relationship between the quality of care (QoC) in the intensive care unit (ICU) and both HRQoL and RtW in ARDS survivors. Therefore, the aim of our study was to investigate associations between indicators of QoC and HRQoL and RtW in a cohort of survivors of ARDS.
Methods: To determine the influence of QoC on HRQoL and RtW 1 year after ICU-discharge, ARDS patients were recruited into a prospective multi-centre patient cohort study and followed up regularly after discharge. Patients were asked to complete self-report questionnaires on HRQoL (Short Form 12 physical component scale (PCS) and mental component scale (MCS)) and RtW. Indicators of QoC pertaining to volume, structural and process quality, and general characteristics were recorded on ICU level. Associations between QoC indicators and HrQoL and RtW were investigated by multivariable linear and Cox regression modelling, respectively. B values and hazard ratios (HRs) are reported with corresponding 95% confidence intervals (CIs).
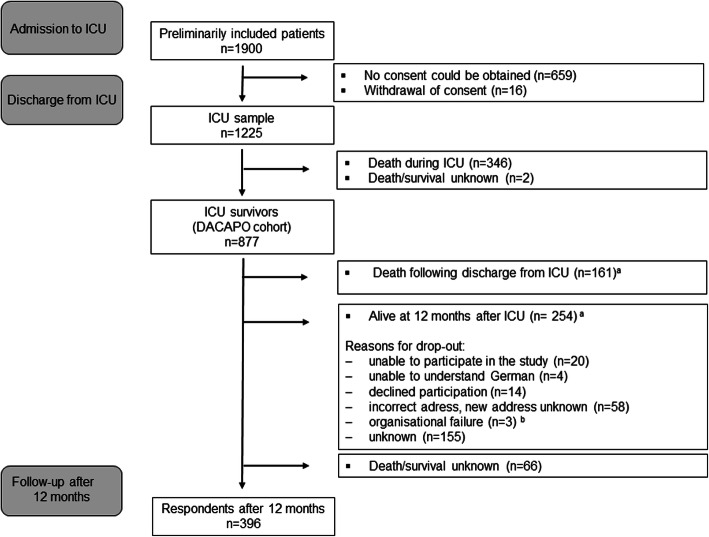
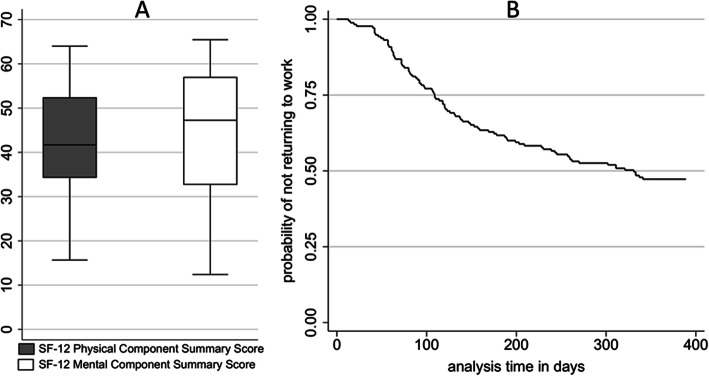
Results: 877 (of initially 1225 enrolled) people with ARDS formed the DACAPO survivor cohort, 396 were finally followed up to 1 year after discharge. The twelve-month survivors were characterized by a reduced HRQoL with a greater impairment in the physical component (Md 41.2 IQR [34-52]) compared to the mental component (Md 47.3 IQR [33-57]). Overall, 50% of the patients returned to work. The proportion of ventilated ICU patients showed significant negative associations with both 12 months PCS (B = - 11.22, CI -20.71; - 1,74) and RtW (HR = 0,18, CI 0,04;0,80). All other QoC indicators were not significantly related to outcome.
Conclusions: Associations between ICU QoC and long-term HrQoL and RtW were weak and largely non-significant. Residual confounding by case mix, treatment variables before or during ICU stay and variables pertaining to the post intensive care period (e.g. rehabilitation) cannot be ruled out.
Trial registration: Clinicaltrials.govNCT02637011. (December 22, 2015, retrospectively registered).
Keywords: ARDS; Health-related quality of life; ICU; Quality of care; Return to work; Volume.
Conflict of interest statement
TB, CK, MQ, SK, CP, SB3, BE, TK, CA2, PM, and SWC are members of the German ARDS-Network. TB: received honoraria for lectures from Xenios Company, Germany. MQ: received honoraria for lectures from Maquet, Company, and Xenios Company, Germany. All other authors declare: no relationships/conditions/circumstances that present a potential conflict of interest.
Figures
References
-
- Marti J, Hall P, Hamilton P, Lamb S, McCabe C, Lall R, et al. One-year resource utilisation, costs and quality of life in patients with acute respiratory distress syndrome (ARDS): secondary analysis of a randomised controlled trial. J Intensive Care. 2016;4:56. doi: 10.1186/s40560-016-0178-8. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
