

Portosystemic shunt surgery in the era of TIPS: imaging-based planning of the surgical approach
- PMID: 32504130
- PMCID: PMC8197708
- DOI: 10.1007/s00261-020-02599-z
Portosystemic shunt surgery in the era of TIPS: imaging-based planning of the surgical approach
Erratum in
-
Correction to: Portosystemic shunt surgery in the era of TIPS: imaging‑based planning of the surgical approach.Abdom Radiol (NY). 2021 Oct;46(10):5053. doi: 10.1007/s00261-021-03153-1. Abdom Radiol (NY). 2021. PMID: 34156510 Free PMC article. No abstract available.
Abstract
Purpose: With the spread of transjugular intrahepatic portosystemic shunts (TIPS), portosystemic shunt surgery (PSSS) has decreased and leaves more complex patients with great demands for accurate preoperative planning. The aim was to evaluate the role of imaging for predicting the most suitable PSSS approach.
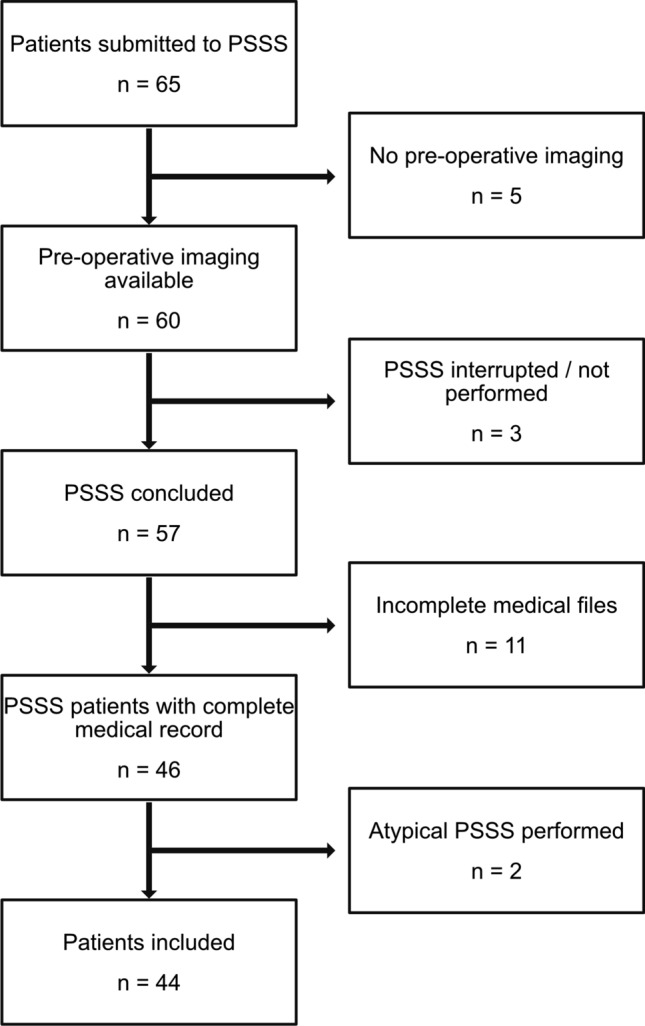
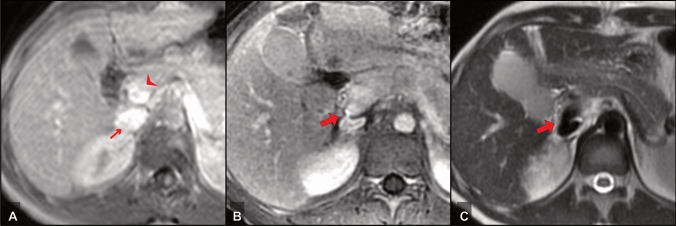
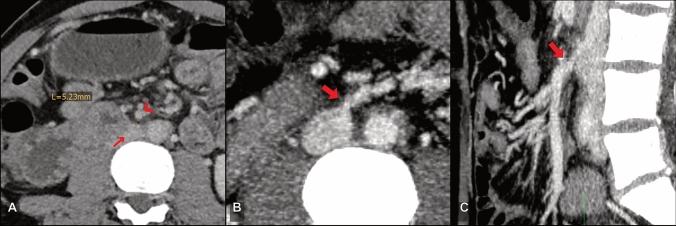
Material and methods: Forty-four patients who underwent PSSS (2002 to 2013) were examined by contrast-enhanced CT (n = 33) and/or MRI (n = 15) prior to surgery. Imaging was analyzed independently by two observers (O1 and O2) with different levels of experience (O1 > O2). They recommended two shunting techniques (vessels and anastomotic variant) for each patient and ranked them according to their appropriateness and complexity. Findings were compared with the actually performed shunt procedure and its outcome.
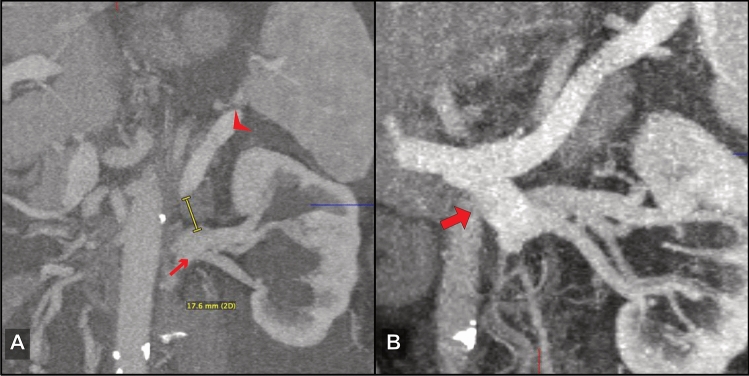
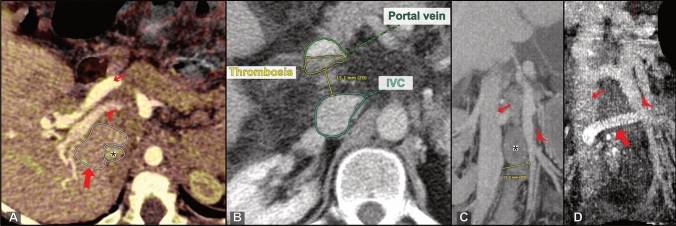
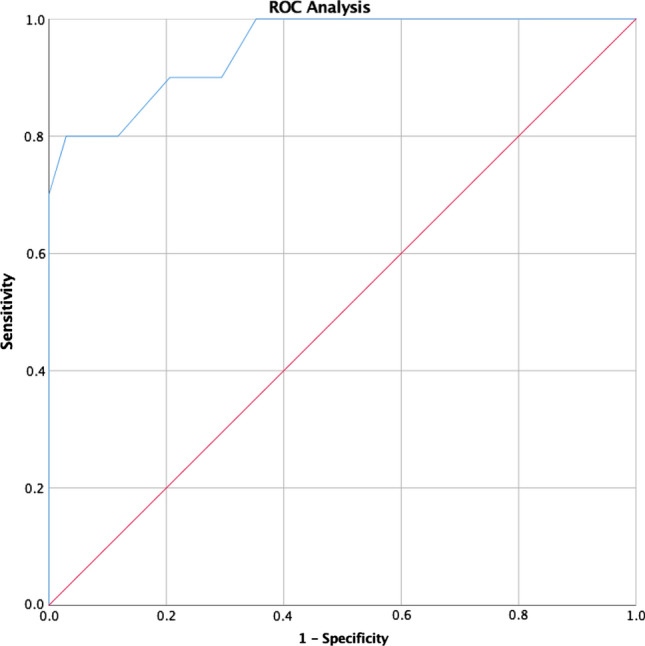
Results: The first two choices taken together covered the performed PSSS regarding vessels in 88%/100% (CT/MRI, O1) and 76%/73% (O2); and vessels + anastomosis in 79%/73% (O1) and 67%/60% (O2). The prediction of complex surgical procedures (resection of interposing structures, additional thrombectomy, use of a collateral vessel, and use of a graft interposition) was confirmed in 87%, resulting in 80% sensitivity and 96% specificity. Larger shunt vessel distances were associated with therapy failure (p = 0.030) and a vessel distance of ≥ 20 mm was identified as optimal cutoff, in which a graft interposition was used. There was no significant difference between MRI and CT in predicting the intraoperative decisions (p = 0.294 to 1.000).
Conclusion: Preoperative imaging and an experienced radiologist can guide surgeons in PSSS. CT and MRI provide the information necessary to identify technically feasible variants and complicating factors.
Keywords: Computed tomography; Magnetic resonance imaging; Portal hypertension; Portosystemic shunt surgery.
Conflict of interest statement
Research grants: Siemens, b.e. imaging, Guerbet. Travel costs and honoraria: Siemens, Canon, Novartis, IPSEN, b.e. imaging, Bayer, Parexel.
Figures
References
-
- Knechtle SJ, D’Alessandro AM, Armbrust MJ, Musat A, Kalayoglu M (1999) Surgical portosystemic shunts for treatment of portal hypertensive bleeding: outcome and effect on liver function. Surgery 126 (4):708–711; discussion 711–703 - PubMed
-
- Rosemurgy AS, Molloy DL, Thometz DP, Villadolid DV, Cowgill SM, Zervos EE (2007) TIPS in Florida: is its application a result of evidence-based medicine? J Am Coll Surg 204 (5):794–801; discussion 801–792. 10.1016/j.jamcollsurg.2007.01.014 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
