

The medial ligaments and the ACL restrain anteromedial laxity of the knee
- PMID: 32504158
- PMCID: PMC7669770
- DOI: 10.1007/s00167-020-06084-4
The medial ligaments and the ACL restrain anteromedial laxity of the knee
Abstract
Purpose: The purpose of this study was to determine the contribution of each of the ACL and medial ligament structures in resisting anteromedial rotatory instability (AMRI) loads applied in vitro.
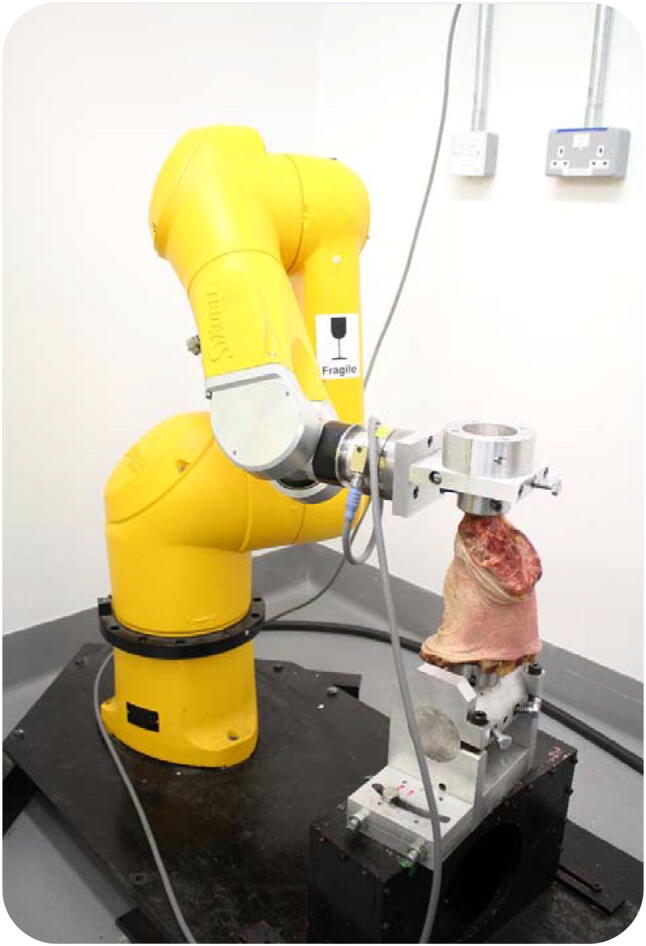
Methods: Twelve knees were tested using a robotic system. It imposed loads simulating clinical laxity tests at 0° to 90° flexion: ±90 N anterior-posterior force, ±8 Nm varus-valgus moment, and ±5 Nm internal-external rotation, and the tibial displacements were measured in the intact knee. The ACL and individual medial structures-retinaculum, superficial and deep medial collateral ligament (sMCL and dMCL), and posteromedial capsule with oblique ligament (POL + PMC)-were sectioned sequentially. The tibial displacements were reapplied after each cut and the reduced loads required allowed the contribution of each structure to be calculated.
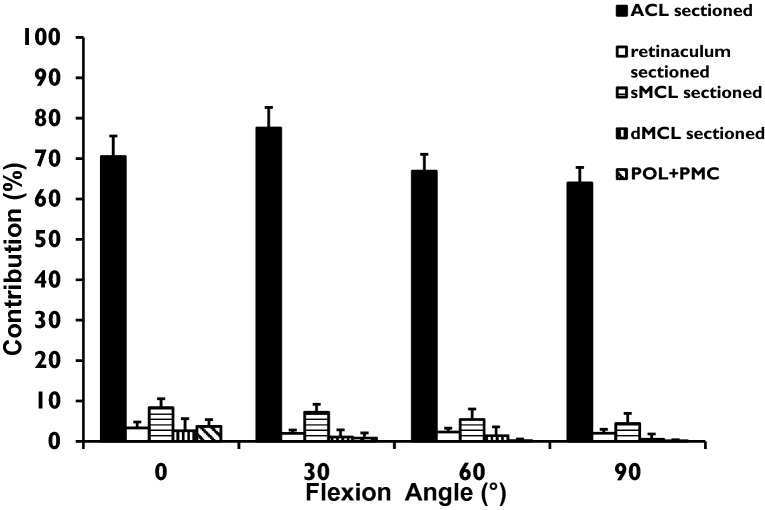
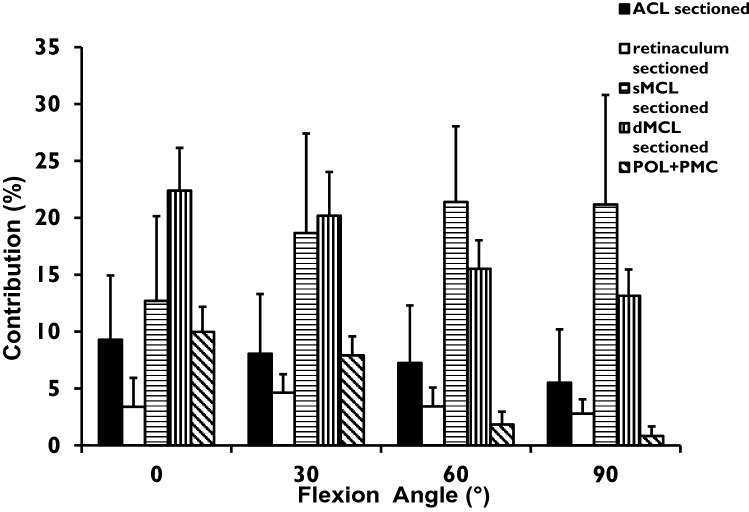
Results: For anterior translation, the ACL was the primary restraint, resisting 63-77% of the drawer force across 0° to 90°, the sMCL contributing 4-7%. For posterior translation, the POL + PMC contributed 10% of the restraint in extension; other structures were not significant. For valgus load, the sMCL was the primary restraint (40-54%) across 0° to 90°, the dMCL 12%, and POL + PMC 16% in extension. For external rotation, the dMCL resisted 23-13% across 0° to 90°, the sMCL 13-22%, and the ACL 6-9%.
Conclusion: The dMCL is the largest medial restraint to tibial external rotation in extension. Therefore, following a combined ACL + MCL injury, AMRI may persist if there is inadequate healing of both the sMCL and dMCL, and MCL deficiency increases the risk of ACL graft failure.
Keywords: Anterior cruciate ligament; Anteromedial rotatory instability; Biomechanics; Medial collateral ligament; Posterior oblique ligament; Restraint of tibiofemoral joint laxity.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures


References
-
- Amis AA (1999) The kinematics of knee stability. In: Jakob RP, Fulford P, Horan F (eds) EFORT European instructional course lectures. vol 4. J Bone Joint Surg Lond, p 96–104
MeSH terms
LinkOut - more resources
Full Text Sources
