

Detection of SARS-CoV-2 antibodies using commercial assays and seroconversion patterns in hospitalized patients
- PMID: 32504735
- PMCID: PMC7834649
- DOI: 10.1016/j.jinf.2020.05.077
Detection of SARS-CoV-2 antibodies using commercial assays and seroconversion patterns in hospitalized patients
Abstract
Objectives: SARS-CoV-2 antibody assays are needed for serological surveys and as a complement to molecular tests to confirm COVID-19. However, the kinetics of the humoral response against SARS-CoV-2 remains poorly described and relies on the performance of the different serological tests.
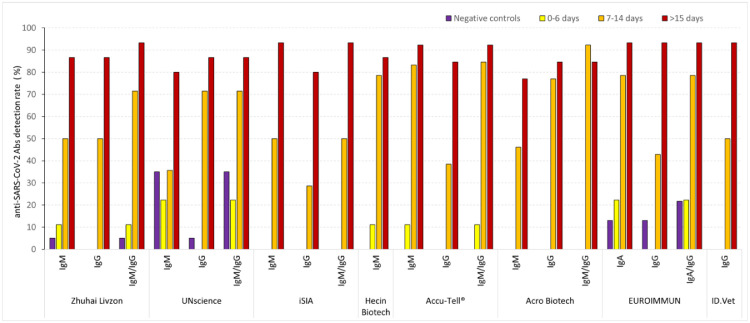
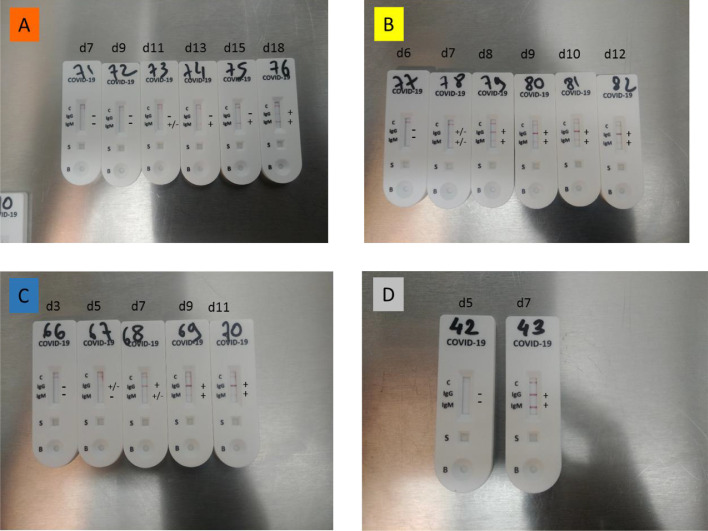
Methods: In this study, we evaluated the performance of six CE-marked point-of-care tests (POC) and three ELISA assays for the diagnosis of COVID-19 by exploring seroconversions in hospitalized patients who tested positive for SARS-CoV-2 RNA.
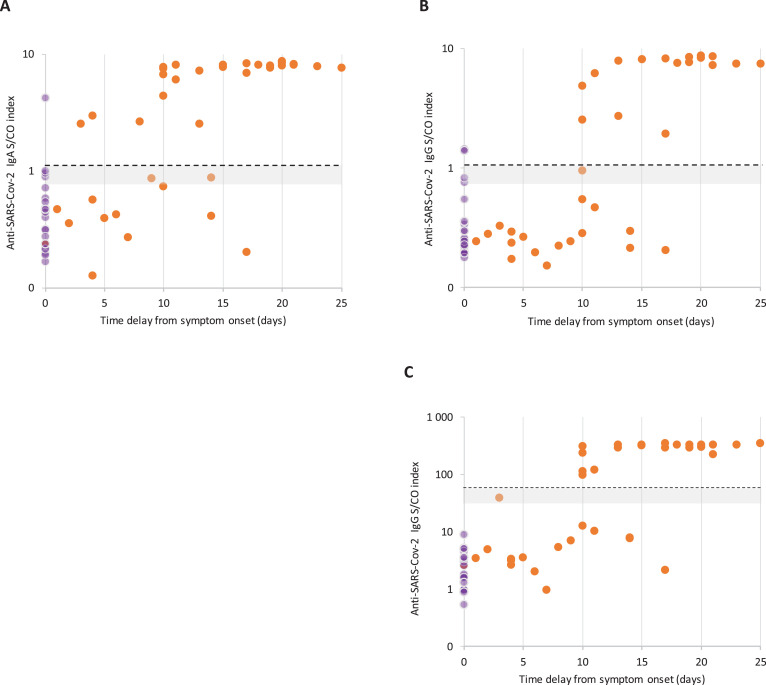
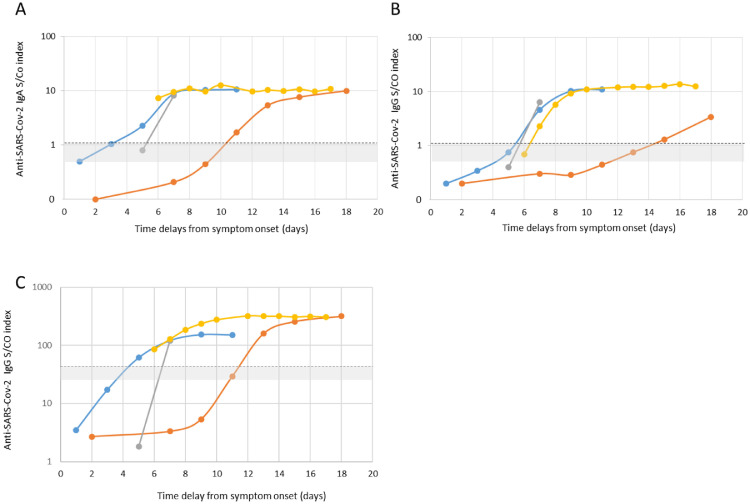
Results: Both the ELISA and POC tests were able to detect SARS-CoV-2 antibodies in at least half of the samples collected seven days or more after the onset of symptoms. After 15 days, the rate of detection rose to over 80% but without reaching 100%, irrespective of the test used. More than 90% of the samples collected after 15 days tested positive using the iSIA and Accu-Tell® POC tests and the ID.Vet IgG ELISA assay. Seroconversion was observed 5 to 12 days after the onset of symptoms. Three assays suffer from a specificity below 90% (EUROIMMUN IgG and IgA, UNscience, Zhuhai Livzon).
Conclusions: The second week of COVID-19 seems to be the best period for assessing the sensitivity of commercial serological assays. To achieve an early diagnosis of COVID-19 based on antibody detection, a dual challenge must be met: the immunodiagnostic window period must be shortened and an optimal specificity must be conserved.
Keywords: COVID-19; ELISA; SARS-CoV-2 antibodies; point of care tests.
Copyright © 2020. Published by Elsevier Ltd.
Conflict of interest statement
Conflict of Interest The authors declare that there are no conflicts of interest.
Figures
Comment in
-
Kinetics and performance of the Abbott architect SARS-CoV-2 IgG antibody assay.J Infect. 2020 Dec;81(6):e7-e9. doi: 10.1016/j.jinf.2020.07.031. Epub 2020 Jul 30. J Infect. 2020. PMID: 32739487 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
