

High SARS-CoV-2 antibody prevalence among healthcare workers exposed to COVID-19 patients
- PMID: 32504745
- PMCID: PMC7270786
- DOI: 10.1016/j.jinf.2020.05.067
High SARS-CoV-2 antibody prevalence among healthcare workers exposed to COVID-19 patients
Abstract
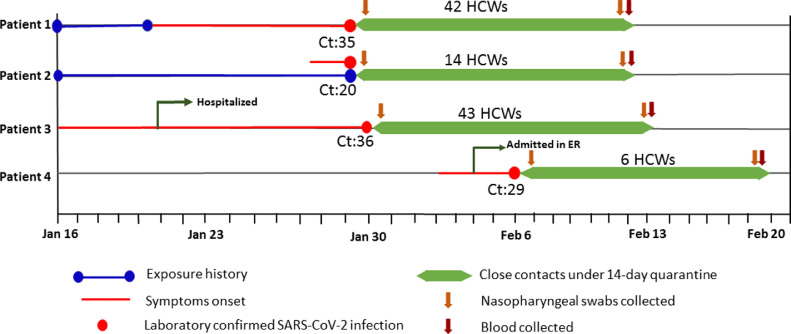
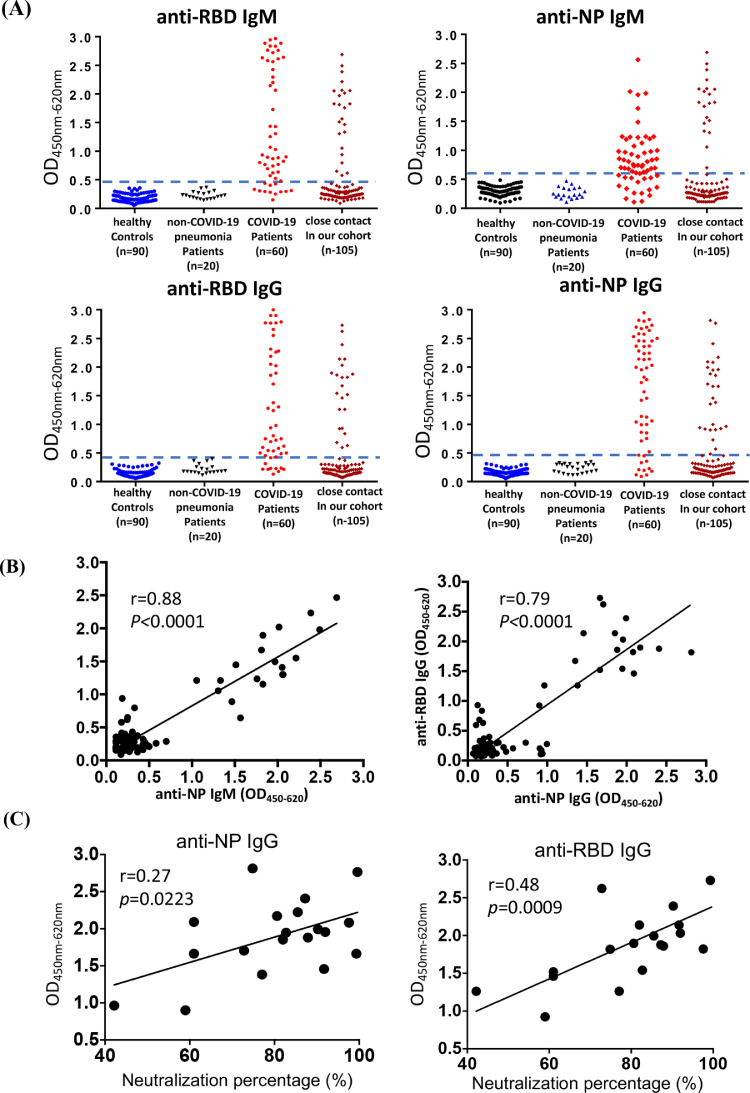
The seroprevalence of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was examined among 105 healthcare workers (HCWs) exposed to four patients who were laboratory confirmed with coronavirus disease 2019 (COVID-19), the disease caused by SARS-CoV-2 infection. These HCWs were immediately under quarantine for 14 days as soon as they were identified as close contacts. The nasopharyngeal swab samples were collected on the first and 14th day of the quarantine, while the serum samples were obtained on the 14th day of the quarantine. With the assay of enzyme immunoassay (EIA) and microneutralization assay, 17.14% (18/105) of HCWs were seropositive, while their swab samples were found to be SARS-CoV-2 RNA negative. Risk analysis revealed that wearing face mask could reduce the infection risk (odds ratio [OR], 0.127, 95% confidence interval [CI] 0.017, 0.968), while when exposed to COVID-19 patients, doctors might have higher risk of seroconversion (OR, 346.837, 95% CI 8.924, 13479.434), compared with HCWs exposed to colleagues as well as nurses and general service assistants who exposed to patients. Our study revealed that the serological testing is useful for the identification of asymptomatic or subclinical infection of SARS-CoV-2 among close contacts with COVID-19 patients.
Keywords: COVID-19; Healthcare workers; Risk factors; SARS-CoV-2; Seroprevalence.
Copyright © 2020 The British Infection Association. Published by Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors have declared that no conflicts of interest.
Figures
Comment in
-
High SARS-CoV-2 infection rates in respiratory staff nurses and correlation of COVID-19 symptom patterns with PCR positivity and relative viral loads.J Infect. 2020 Sep;81(3):452-482. doi: 10.1016/j.jinf.2020.06.035. Epub 2020 Jun 18. J Infect. 2020. PMID: 32562793 Free PMC article. No abstract available.
-
Letter in response to article in journal of infection: "High SARS-CoV-2 antibody prevalence among healthcare workers exposed to COVID-19 patients".J Infect. 2020 Sep;81(3):e26-e28. doi: 10.1016/j.jinf.2020.07.001. Epub 2020 Jul 3. J Infect. 2020. PMID: 32628961 Free PMC article. No abstract available.
-
Immunological detection of serum antibodies in pediatric medical workers exposed to varying levels of SARS-CoV-2.J Infect. 2021 Jan;82(1):159-198. doi: 10.1016/j.jinf.2020.07.023. Epub 2020 Jul 25. J Infect. 2021. PMID: 32721505 Free PMC article. No abstract available.
-
Large-scale, molecular and serological SARS-CoV-2 screening of healthcare workers in a 4-site public hospital in Belgium after COVID-19 outbreak.J Infect. 2021 Jan;82(1):159-198. doi: 10.1016/j.jinf.2020.07.033. Epub 2020 Jul 31. J Infect. 2021. PMID: 32739485 Free PMC article. No abstract available.
-
The implementation of an active surveillance integrating information technology and drive-through coronavirus testing station for suspected COVID-19 cases.J Infect. 2021 Feb;82(2):282-327. doi: 10.1016/j.jinf.2020.08.051. Epub 2020 Sep 3. J Infect. 2021. PMID: 32890596 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
