

A randomized, open-label, Phase III study of obinutuzumab or rituximab plus CHOP in patients with previously untreated diffuse large B-Cell lymphoma: final analysis of GOYA
- PMID: 32505213
- PMCID: PMC7276080
- DOI: 10.1186/s13045-020-00900-7
A randomized, open-label, Phase III study of obinutuzumab or rituximab plus CHOP in patients with previously untreated diffuse large B-Cell lymphoma: final analysis of GOYA
Abstract
Background: Rituximab (R) plus cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP) is the current standard therapy for diffuse large B cell lymphoma (DLBCL). Obinutuzumab (G), a glycoengineered, type II anti-CD20 monoclonal antibody, has shown activity and an acceptable safety profile when combined with CHOP (G-CHOP) in patients with advanced DLBCL. We present the final analysis results of the Phase III GOYA study (NCT01287741), which compared the efficacy and safety of G-CHOP versus R-CHOP in patients with previously untreated DLBCL.
Methods: Patients aged ≥ 18 years with previously untreated advanced DLBCL were randomly assigned to receive eight 21-day cycles of R or G, plus six or eight cycles of CHOP. The primary endpoint was investigator-assessed progression-free survival (PFS). Secondary endpoints included overall survival, other time-to-event endpoints, and safety; investigator-assessed PFS by cell of origin subgroup was an exploratory endpoint.
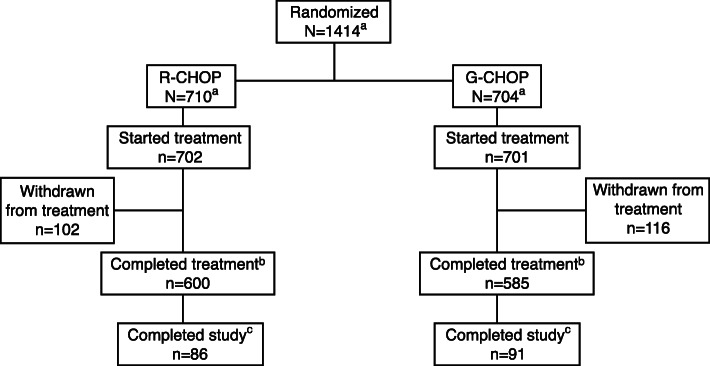
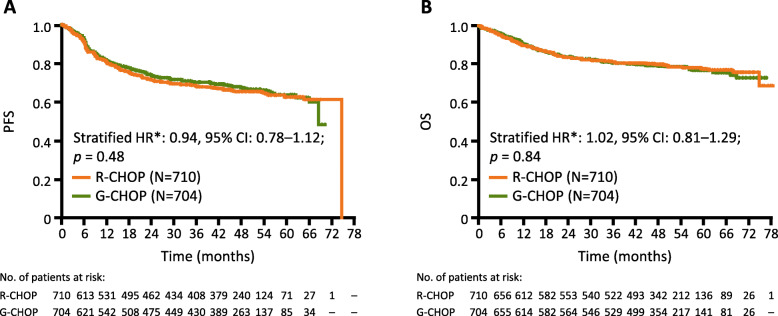
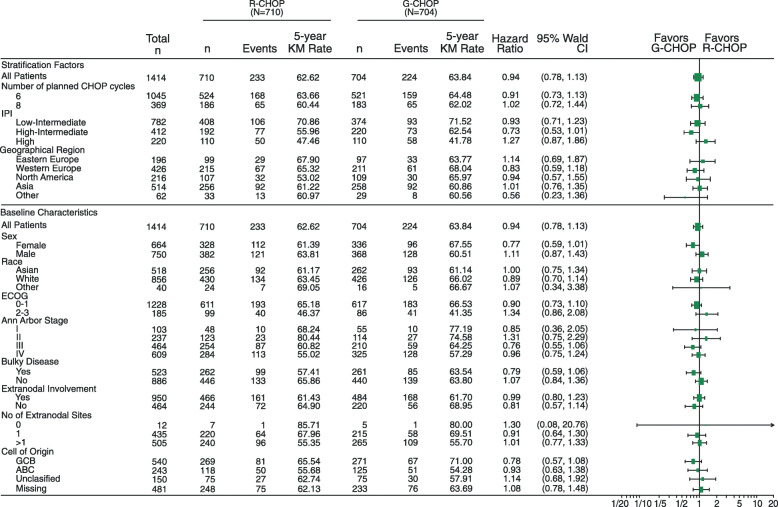
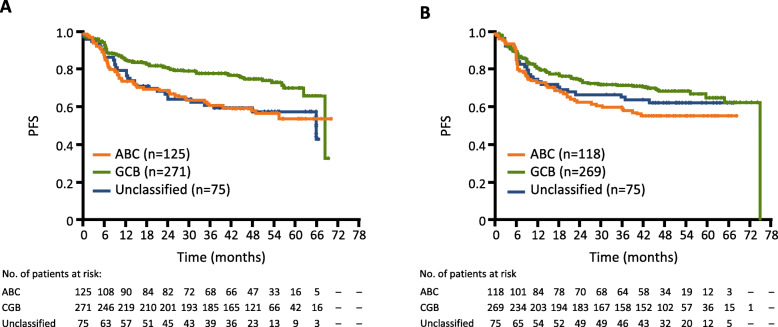
Results: A total of 1418 patients were randomized, with 1414 included in this final analysis (G-CHOP, N = 704; R-CHOP, N = 710). Five-year PFS rates were 63.8% and 62.6% for G-CHOP and R-CHOP, respectively (stratified hazard ratio 0.94, 95% CI 0.78-1.12; p = 0.48). The results of the secondary efficacy endpoints did not show a benefit of G-CHOP over R-CHOP. In the exploratory analysis, a trend towards benefit with G-CHOP over R-CHOP was apparent in the patients with germinal center B cell DLBCL. The safety profile of G-CHOP was as expected, and no new safety signals were observed. More grade 3-5 (75.1% vs 65.8%), serious (44.4% vs 38.4%), and fatal (6.1% vs 4.4%) adverse events (AEs) were observed in the G-CHOP arm compared with the R-CHOP arm, respectively, with the most common fatal AEs being infections. A higher incidence of late-onset neutropenia occurred in the G-CHOP arm (8.7%) versus the R-CHOP arm (4.9%).
Conclusions: The final analysis, similar to the primary analysis, did not show a PFS benefit of G-CHOP over R-CHOP in previously untreated patients with DLBCL. The results of the secondary endpoints were consistent with the primary endpoint. Further exploratory analyses and investigation of biomarkers are ongoing.
Keywords: Diffuse large B cell lymphoma; Immunochemotherapy; Obinutuzumab; Outcomes; Rituximab.
Conflict of interest statement
C.B is employed by Genentech, Inc. and has equity ownership interests (including stock options) in F. Hoffmann-La Roche. A.K and W.L are employed by F. Hoffmann-La Roche. M.M has received honoraria from F. Hoffmann-La Roche, Celgene, Janssen, Sandoz, Novartis, Gilead, and Servier and is a member of an entity’s Board of Directors or advisory committees for F. Hoffmann-La Roche, Celgene, Janssen, Sandoz, Novartis, and Gilead. D.S and G.S are employed by and have equity ownership interests (including stock options) for F. Hoffmann-La Roche. L.S has provided consultancy (including expert testimony) for F. Hoffmann-La Roche, Genentech, Inc., AbbVie, Amgen, Apobiologix, AstraZeneca, Acerta, Celgene, Gilead, Janssen, Kite, Karyopharm, Lundbeck, Merck, Morphosys, Seattle Genetics, Teva, Takeda, TG Therapeutics, Verastem; has received research funding from F. Hoffmann-La Roche and Genentech, Inc.; and has received honoraria from F. Hoffmann-La Roche, Genentech, Inc., AbbVie, Amgen, Apobiologix, AstraZeneca, Acerta, Celgene, Gilead, Janssen, Kite, Karyopharm, Lundbeck, Merck, MorphoSys, Seattle Genetics, Teva, Takeda, TG Therapeutics, Verastem. M.T provides consultancy (including expert testimony) for Takeda, Bristol-Myers Squibb, Incyte, AbbVie, Amgen, F. Hoffmann-La Roche, Gilead Sciences, Janssen, Celgene, and MorphoSys and has received honoraria from Janssen, Gilead Sciences, Takeda, Bristol-Myers Squibb, Amgen, AbbVie, F. Hoffmann-La Roche, MorphoSys, and Incyte. U.V is part of the speaker’s bureau for Celgene, F. Hoffmann-La Roche, Janssen, Gilead, AbbVie, and Novartis and a member of advisory committees for Janssen, Celgene, Kite, Juno Therapeutics, Gilead, and Novartis.
Figures
References
-
- NCCN Clinical Practice Guidelines in oncology: B-Cell Lymphomas, version 7. 2019 [Accessed 16 January 2020]. Available from: https://www.nccn.org/professionals/physician_gls/pdf/b-cell.pdf.
-
- Herter S, Herting F, Mundigl O, Waldhauer I, Weinzierl T, Fauti T, et al. Preclinical activity of the type II CD20 antibody GA101 (obinutuzumab) compared with rituximab and ofatumumab in vitro and in xenograft models. Mol Cancer Ther. 2013;12(10):2031–2042. doi: 10.1158/1535-7163.MCT-12-1182. - DOI - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
