

Role of Rehabilitation Department for Adult Individuals With COVID-19: The Experience of the San Raffaele Hospital of Milan
- PMID: 32505489
- PMCID: PMC7272153
- DOI: 10.1016/j.apmr.2020.05.015
Role of Rehabilitation Department for Adult Individuals With COVID-19: The Experience of the San Raffaele Hospital of Milan
Abstract
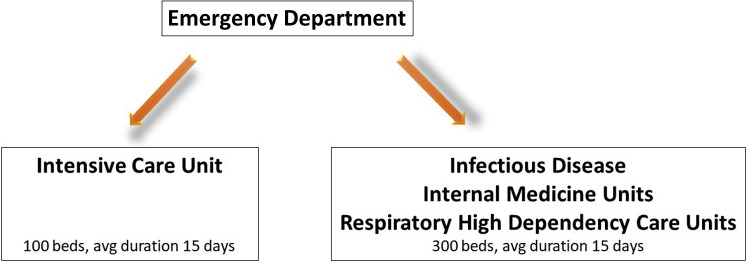
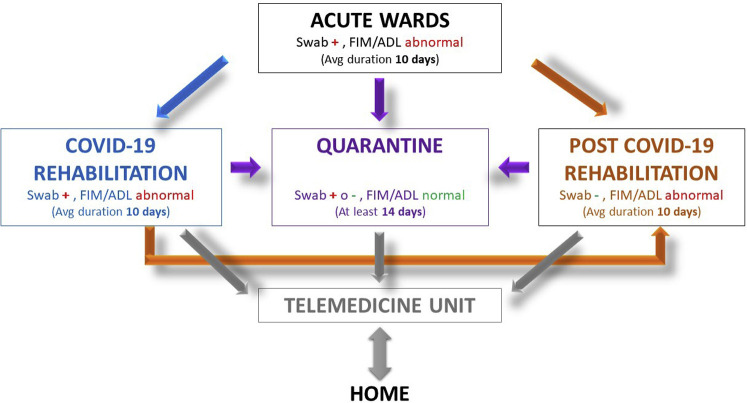
The rapid evolution of the health emergency linked to the spread of severe acute respiratory syndrome coronavirus 2 requires specifications for the rehabilitative management of patients with coronavirus disease 2019 (COVID-19). The symptomatic evolution of patients with COVID-19 is characterized by 2 phases: an acute phase in which respiratory symptoms prevail and a postacute phase in which patients can show symptoms related to prolonged immobilization, to previous and current respiratory dysfunctions, and to cognitive and emotional disorders. Thus, there is the need for specialized rehabilitative care for these patients. This communication reports the experience of the San Raffaele Hospital of Milan and recommends the setup of specialized clinical pathways for the rehabilitation of patients with COVID-19. In this hospital, between February 1 and March 2, 2020, about 50 patients were admitted every day with COVID-19 symptoms. In those days, about 400 acute care beds were created (intensive care/infectious diseases). In the following 30 days, from March 2 to mid-April, despite the presence of 60 daily arrivals to the emergency department, the organization of patient flow between different wards was modified, and several different units were created based on a more accurate integration of patients' needs. According to this new organization, patients were admitted first to acute care COVID-19 units and then to COVID-19 rehabilitation units, post-COVID-19 rehabilitation units, and/or quarantine/observation units. After hospital discharge, telemedicine was used to follow-up with patients at home. Such clinical pathways should each involve dedicated multidisciplinary teams composed of pulmonologists, physiatrists, neurologists, cardiologists, physiotherapists, neuropsychologists, occupational therapists, speech therapists, and nutritionists.
Keywords: Coronavirus; Critical pathways; Neuropsychology; Physical therapy modalities; Rehabilitation; Telemedicine.
Copyright © 2020 American Congress of Rehabilitation Medicine. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Brugliera L., Spina A., Castellazzi P., et al. Rehabilitation of COVID-19 patients. J. Rehabil Med. 2020;52 - PubMed
-
- Kallet R.H., Hemphill J.C., Dicker R.A., et al. The spontaneous breathing pattern and work of breathing of patients with acute respiratory distress syndrome and acute lung injury. Respir Care. 2007;52:989–995. - PubMed
-
- Guérin C., Reignier J., Richard J.-C., et al. Prone positioning in severe acute respiratory distress syndrome. N Engl J Med. 2013;368:2159–2168. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
