

SARS-CoV-2 antibody characterization in emergency department, hospitalized and convalescent patients by two semi-quantitative immunoassays
- PMID: 32505774
- PMCID: PMC7272145
- DOI: 10.1016/j.cca.2020.06.004
SARS-CoV-2 antibody characterization in emergency department, hospitalized and convalescent patients by two semi-quantitative immunoassays
Abstract
Background: In the ongoing COVID-19 pandemic, there is an urgent need for comprehensive performance evaluation and clinical utility assessment of serological assays to understand the immune response to SARS-CoV-2.
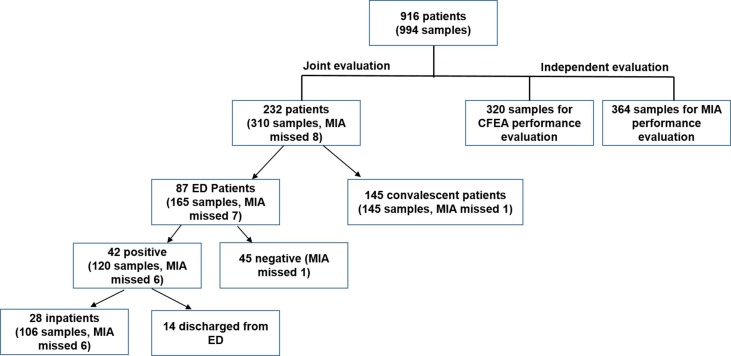
Methods: IgM/IgG and total antibodies against SARS-CoV-2 were measured by a cyclic enhanced fluorescence assay (CEFA) and a microsphere immunoassay (MIA), respectively. Independent performance evaluation included imprecision, reproducibility, specificity and cross-reactivity (CEFA n = 320, MIA n = 364). Clinical utility was evaluated by both methods in 87 patients at initial emergency department visit, 28 during subsequent hospitalizations (106 serial samples), and 145 convalescent patients. Totally 916 patients and 994 samples were evaluated.
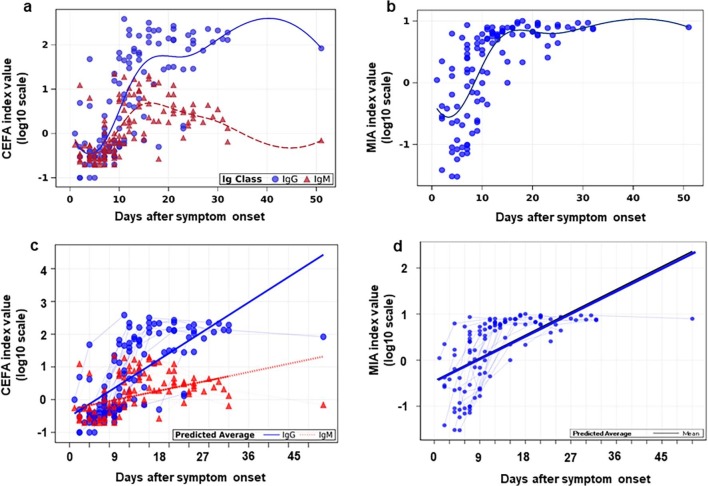
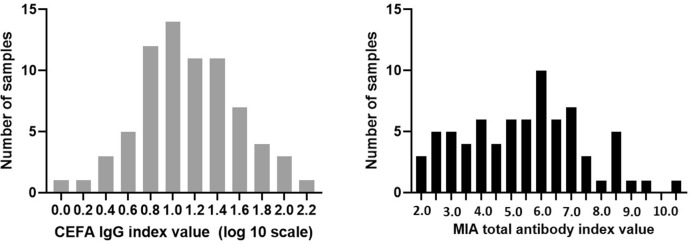
Results: Agreement of CEFA and MIA was 90.4%-94.5% (Kappa: 0.81-0.89) in 302 samples. CEFA and MIA detected SARS-CoV-2 antibodies in 26.2% and 26.3%, respectively, of ED patients. Detection rates increased over time reaching 100% after 21 days post-symptom onset. Longitudinal antibody kinetic changes by CEFA and MIA measurements correlated well and exhibited three types of seroconversion. Convalescent sera showed a wide range of antibody levels.
Conclusion: Rigorously validated CEFA and MIA assays are reliable for detecting antibodies to SARS-CoV-2 and show promising clinical utility when evaluating immune response in hospitalized and convalescent patients, but are not useful for early screening at patient's initial ED visit.
Keywords: Coronavirus disease 19 (COVID-19); Immunoassay; Serology; Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).
Copyright © 2020 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest ZZ received seed instruments and sponsored travel from ET Healthcare. The manufacturers did not review the article and had no input on data analysis prior to the manuscript submission.
Figures


References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
