Effects of the presence of a pediatric intensivist on treatment in the pediatric intensive care unit
- PMID: 32506873
- PMCID: PMC7280800
- DOI: 10.4266/acc.2019.00752
Effects of the presence of a pediatric intensivist on treatment in the pediatric intensive care unit
Abstract
Background: There are few studies on the effect of intensivist staffing in pediatric intensive care units (PICUs) in Korea. We aimed to evaluate the effect of pediatric intensivist staffing on treatment outcomes in a Korean hospital PICU.
Methods: We analyzed two time periods according to pediatric intensivist staffing: period 1, between November 2015 to January 2017 (no intensivist staffing, n=97) and period 2, between February 2017 to February 2018 (intensivists staffing, n=135).
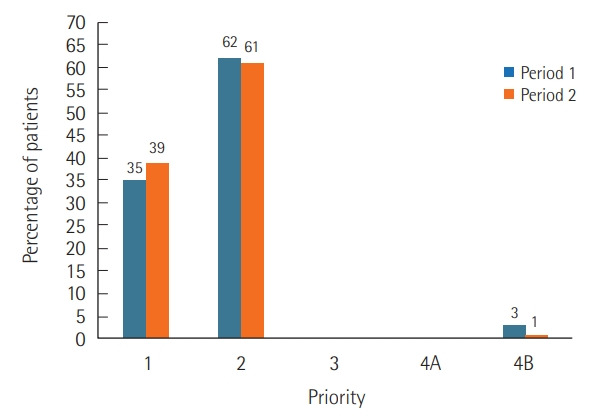
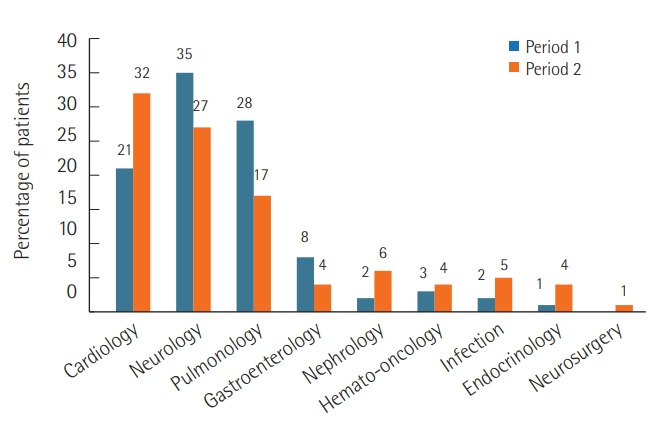
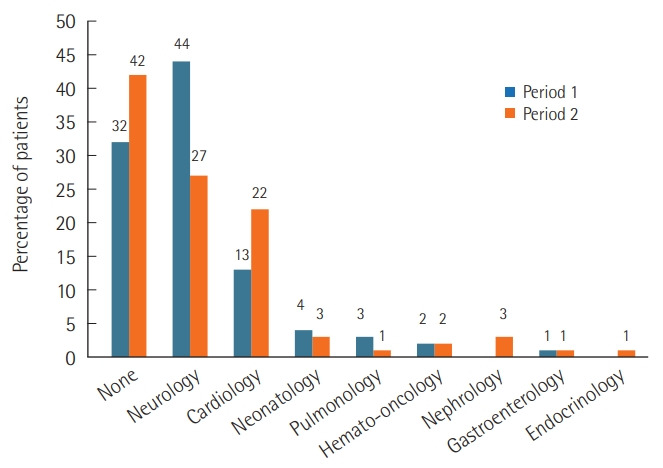
Results: Median age at admission was 5.4 years (range, 0.7-10.3 years) in period 1 and 3.6 years (0.2-5.1 years) in period 2 (P=0.013). The bed occupancy rate decreased in period 2 (75%; 73%-88%) compared to period 1 (89%; 81%-94%; P=0.015). However, the monthly bed turnover rate increased in period 2 (2.2%; 1.9%-2.7%) compared to period 1 (1.5%, 1.1%- 1.7%; P=0.005). In both periods, patients with chronic neurologic illness were the most common. Patients with cardiovascular problems were more prevalent in period 2 than period 1 (P=0.008). Daytime admission occurred more frequently in period 2 than period 1 (63% vs. 39%, P<0.001). The length of PICU stay, parameters related with mechanical ventilation and tracheostomy, and pediatric Sequential Organ Failure Assessment score were not different between periods. Sudden cardiopulmonary resuscitations occurred in two cases during period 1, but no case occurred during period 2.
Conclusions: Pediatric intensivist staffing in the PICU may affect efficient ICU operations.
Keywords: cardiopulmonary resuscitation; child; critical care; intensive care units.
Conflict of interest statement
Figures
References
-
- Pronovost PJ, Angus DC, Dorman T, Robinson KA, Dremsizov TT, Young TL. Physician staffing patterns and clinical outcomes in critically ill patients: a systematic review. JAMA. 2002;288:2151–62. - PubMed
-
- Wilcox ME, Chong CA, Niven DJ, Rubenfeld GD, Rowan KM, Wunsch H, et al. Do intensivist staffing patterns influence hospital mortality following ICU admission? A systematic review and meta-analyses. Crit Care Med. 2013;41:2253–74. - PubMed
-
- Milstein A, Galvin RS, Delbanco SF, Salber P, Buck CR., Jr Improving the safety of health care: the leapfrog initiative. Eff Clin Pract. 2000;3:313–6. - PubMed
-
- Gajic O, Afessa B. Physician staffing models and patient safety in the ICU. Chest. 2009;135:1038–44. - PubMed
-
- Haupt MT, Bekes CE, Brilli RJ, Carl LC, Gray AW, Jastremski MS, et al. Guidelines on critical care services and personnel: recommendations based on a system of categorization of three levels of care. Crit Care Med. 2003;31:2677–83. - PubMed
LinkOut - more resources
Full Text Sources