

The reliability and feasibility of non-contrast adenosine stress cardiovascular magnetic resonance T1 mapping in patients on haemodialysis
- PMID: 32507107
- PMCID: PMC7278072
- DOI: 10.1186/s12968-020-00634-y
The reliability and feasibility of non-contrast adenosine stress cardiovascular magnetic resonance T1 mapping in patients on haemodialysis
Abstract
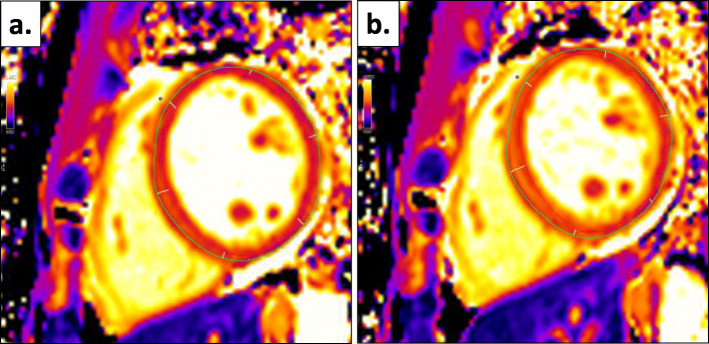
Background: Identifying coronary artery disease (CAD) in patients with end-stage renal disease (ESRD) is challenging. Adenosine stress native T1 mapping with cardiovascular magnetic resonance (CMR) may accurately detect obstructive CAD and microvascular dysfunction in the general population. This study assessed the feasibility and reliability of adenosine stress native T1 mapping in patients on haemodialysis.
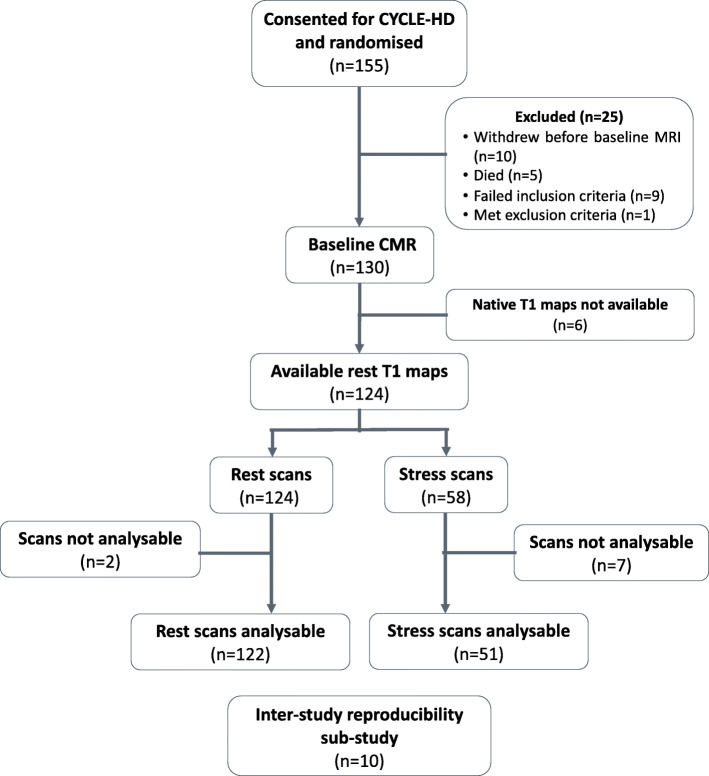
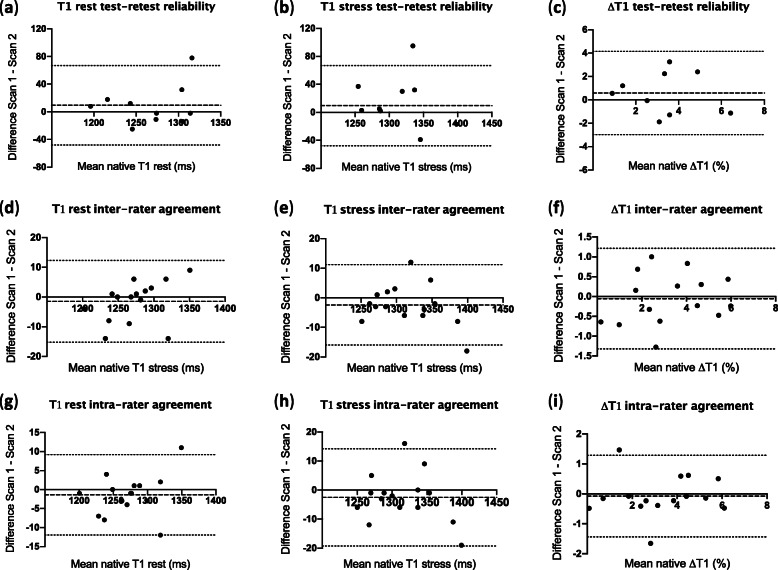
Methods: The feasibility of undertaking rest and adenosine stress native T1 mapping using the single-shot Modified Look-Locker inversion recovery (MOLLI) sequence was assessed in 58 patients on maintenance haemodialysis using 3 T CMR. Ten patients underwent repeat stress CMR within 2 weeks for assessment of test-retest reliability of native T1, stress T1 and delta T1 (ΔT1). Interrater and intrarater agreement were assessed in 10 patients. Exploratory analyses were undertaken to assess associations between clinical variables and native T1 values in 51 patients on haemodialysis.
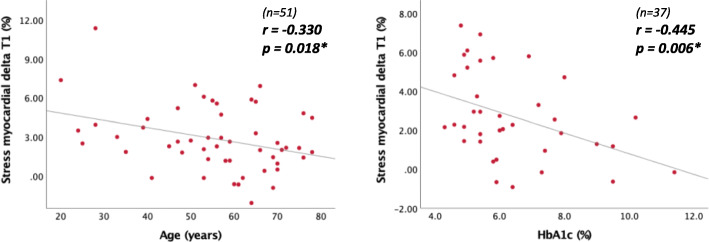
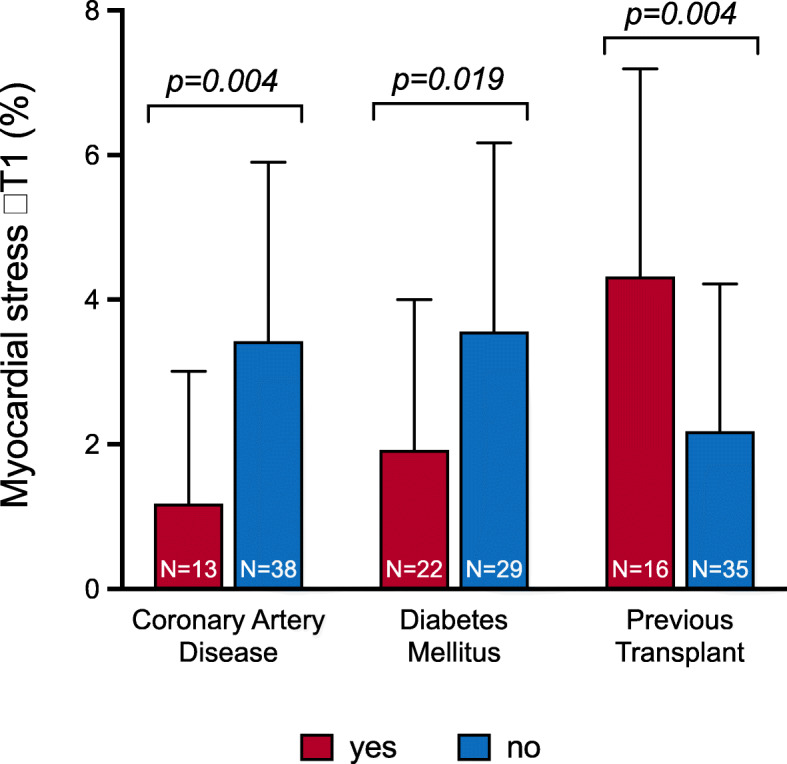
Results: Mean age of participants was 55 ± 15 years, 46 (79%) were male, and median dialysis vintage was 21 (8; 48) months. All patients completed the scan without complications. Mean native T1 rest, stress and ΔT1 were 1261 ± 57 ms, 1297 ± 50 ms and 2.9 ± 2.5%, respectively. Interrater and intrarater agreement of rest T1, stress T1 and ΔT1 were excellent, with intraclass correlation coefficients (ICC) > 0.9 for all. Test-retest reliability of rest and stress native T1 were excellent or good (CoV 1.2 and 1.5%; ICC, 0.79 and 0.69, respectively). Test-retest reliability of ΔT1 was moderate to poor (CoV 27.4%, ICC 0.55). On multivariate analysis, CAD, diabetes mellitus and resting native T1 time were independent determinants of ΔT1 (β = - 0.275, p = 0.019; β = - 0.297, p = 0.013; β = - 0.455; p < 0.001, respectively).
Conclusions: Rest and adenosine stress native T1 mapping is feasible and well-tolerated amongst patients with ESRD on haemodialysis. Although rater agreement of the technique is excellent, test-retest reliability of ΔT1 is moderate to poor. Prospective studies should evaluate the relationship between this technique and established methods of CAD assessment and association with outcomes.
Keywords: Coronary artery disease; End-stage renal disease; Feasibility; Haemodialysis; Myocardial ischaemia; Reliability; Reproducibility; Stress T1.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Nagel E, Greenwood JP, McCann GP, Bettencourt N, Shah AM, Hussain ST, et al. Magnetic resonance perfusion or fractional flow Reserve in Coronary Disease. N Engl J Med. 2019;380(25):2418–2428. - PubMed
-
- von Knobelsdorff-Brenkenhoff F, Schulz-Menger J. Cardiovascular magnetic resonance imaging in ischemic heart disease. J Magn Reson Imaging. 2012;36(1):20–38. - PubMed
-
- Kay J. Nephrogenic systemic fibrosis: a gadolinium-associated fibrosing disorder in patients with renal dysfunction. Ann Rheum Dis. 2008;67(Suppl 3):iii66–iii69. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
