

Long-term opioid use after bariatric surgery
- PMID: 32507657
- PMCID: PMC7423624
- DOI: 10.1016/j.soard.2020.04.037
Long-term opioid use after bariatric surgery
Abstract
Background: Opioid analgesics are often prescribed to manage pain after bariatric surgery, which may develop into chronic prescription opioid use (CPOU) in opioid-naïve patients. Bariatric surgery may affect opioid use in those with or without presurgical CPOU.
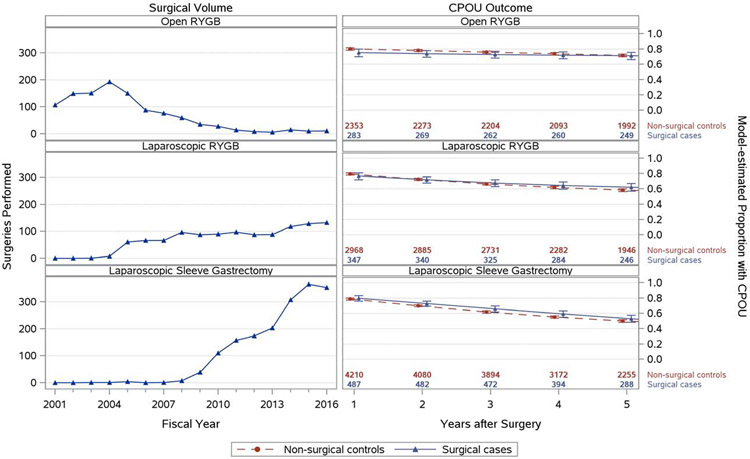
Objective: To compare CPOU persistence and incidence in a large multisite cohort of veterans undergoing bariatric surgery (open Roux-en-Y gastric bypass, laparoscopic RYGB, or laparoscopic sleeve gastrectomy) and matched nonsurgical controls.
Setting: Veterans Administration hospitals.
Methods: In a retrospective cohort study, we matched 1117 surgical patients with baseline CPOU to 9531 nonsurgical controls, and 2822 surgical patients without CPOU at baseline to 26,392 nonsurgical controls using sequential stratification. CPOU persistence in veterans with baseline CPOU was estimated using generalized estimating equations by procedure type. CPOU incidence in veterans without baseline CPOU was estimated in Cox regression models by procedure type because postoperative pain, complications, and absorption may differ by procedure.
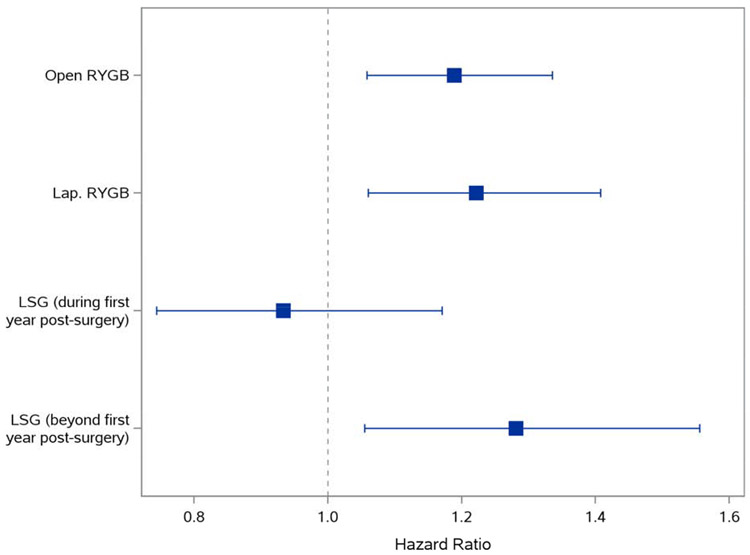
Results: In veterans with baseline CPOU, postsurgical CPOU declined over time for each surgical procedure; these trends did not differ between surgical patients and nonsurgical controls. In veterans without baseline CPOU, compared with nonsurgical controls, bariatric patients had higher CPOU incidence within 5 years after open Roux-en-Y gastric bypass (hazard ratio = 1.19; 95% confidence interval: 1.06-1.34) or laparoscopic open Roux-en-Y gastric bypass (hazard ratio = 1.22, 95% confidence interval: 1.06-1.41). Veterans undergoing laparoscopic sleeve gastrectomy had higher CPOU incidence 1 to 5 years after surgery (hazard ratio = 1.28; 95% confidence interval: 1.05-1.56) than nonsurgical controls.
Conclusions: Bariatric surgery was associated with greater risk of CPOU incidence in patients without baseline CPOU but was not associated with greater CPOU persistence.
Keywords: Bariatric; Gastric bypass; Matching; Medication; Obesity; Opioid; Sleeve gastrectomy; Surgery; Veterans.
Published by Elsevier Inc.
Conflict of interest statement
Figures

References
-
- Trescot AM, Helm S, Hansen H, et al. Opioids in the management of chronic non-cancer pain: an update of American Society of the Interventional Pain Physicians’ (ASIPP) Guidelines. Pain Physician. 2008;11(2 Suppl):S5–S62. - PubMed
-
- Turk DC, Wilson HD, Cahana A. Treatment of chronic non-cancer pain. Lancet. 2011. ;377(9784):2226–2235. - PubMed
-
- Paulozzi LJ, Weisler RH, Patkar AA. A national epidemic of unintentional prescription opioid overdose deaths: how physicians can help control it. J Clin Psychiatry. 2011. ;72(5):589–592. - PubMed
-
- Han B, Compton WM, Blanco C, Crane E, Lee J, Jones CM. Prescription Opioid Use, Misuse, and Use Disorders in U.S. Adults: 2015 National Survey on Drug Use and Health. Ann Intern Med. 2017;167(5):293–301. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
