

Mapping endocrine toxicity spectrum of immune checkpoint inhibitors: a disproportionality analysis using the WHO adverse drug reaction database, VigiBase
- PMID: 32507965
- PMCID: PMC7447663
- DOI: 10.1007/s12020-020-02355-9
Mapping endocrine toxicity spectrum of immune checkpoint inhibitors: a disproportionality analysis using the WHO adverse drug reaction database, VigiBase
Abstract
Purpose: Our study aimed to map endocrine toxicity spectrum of immune checkpoint inhibitors (ICIs).
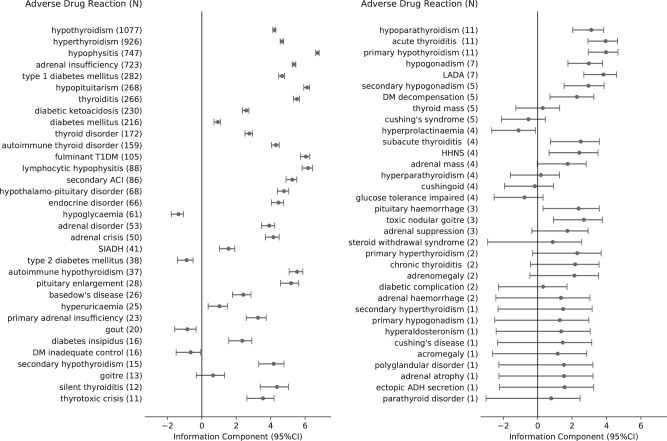
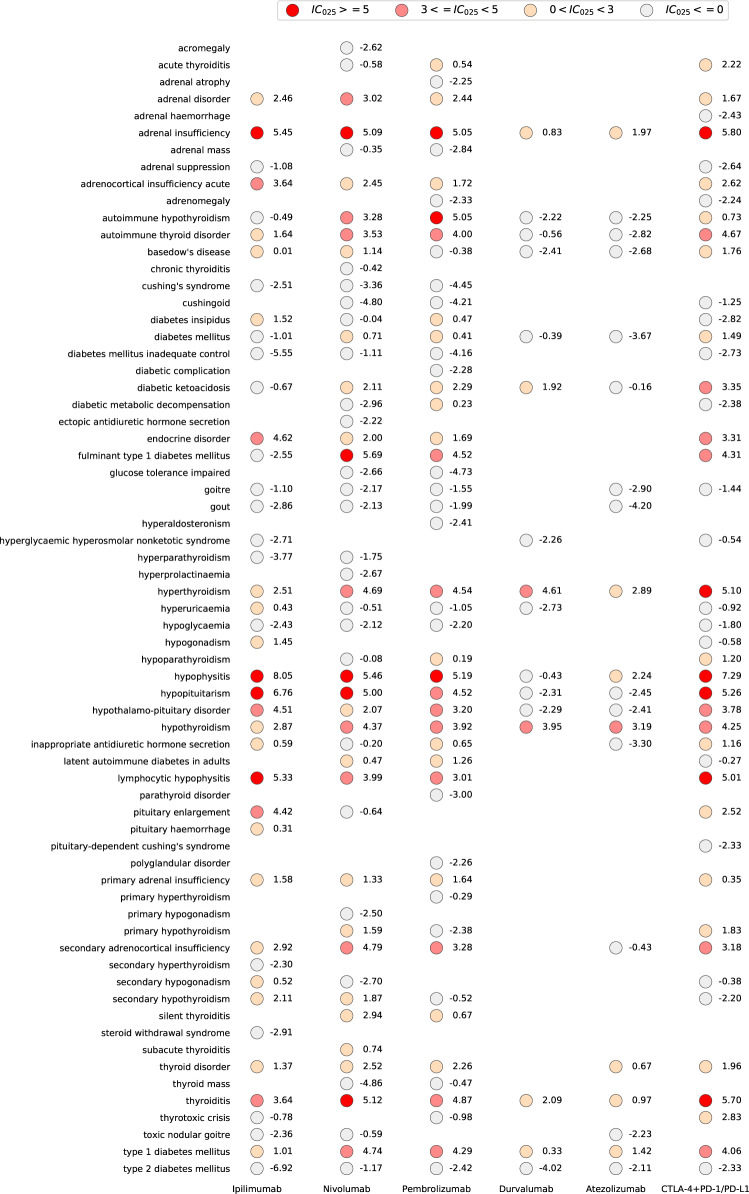
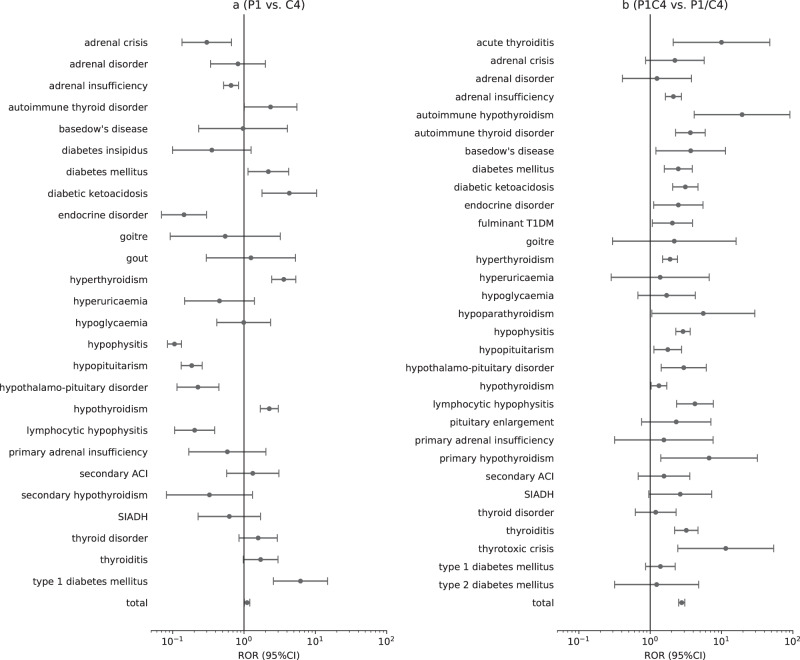
Methods: We obtained data from VigiBase, between January 1, 2011 and March 6, 2019. All endocrine adverse drug reactions (ADRs) were classified by group queries according to the Medical Dictionary for Regulatory Activities. Disproportionality analysis was performed with information component (IC) and reporting odds ratio (ROR). We used IC to identify meaningful endocrinopathies associated with ICIs and ROR to compare differences between ICI subgroups of ADRs. IC025 (lower end of the 95% confidence interval of IC) is considered significant if larger than 0.
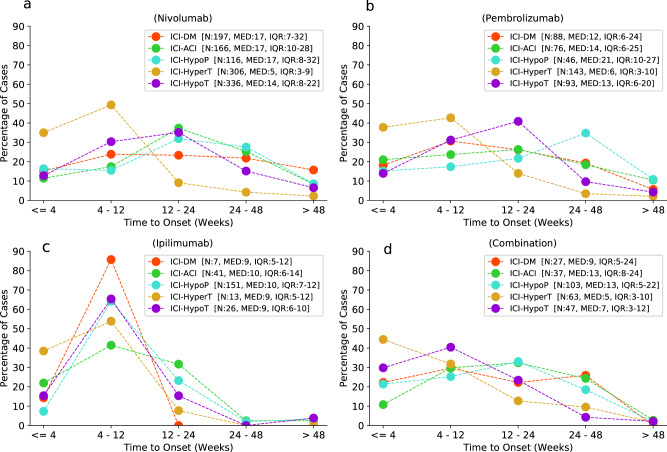
Results: In all, 6089 reports for endocrinopathies associated with ICIs were involved, with a male to female ratio of 1.5:1. The disproportionality analysis indicated significance of not only common endocrinopathies: thyroid dysfunction, hypophysitis/hypopituitarism, adrenal insufficiency, T1DM, fulminant T1DM (IC025: 4.12-6.62), but also rare endocrinopathies: hypoparathyroidism, diabetes insipidus, hypogonadism (IC025: 1.56-2.04). Increased risk of ADR reporting emerged in anti-CTLA-4 (e.g., hypophysitis/hypopituitarism, adrenal insufficiency) or in anti-PD-1/PD-L1 (e.g., thyroid dysfunction, T1DM, fulminant T1DM). In general, combination therapy (anti-CTLA-4 plus anti-PD-1/PD-L1) had a stronger association with endocrinopathies than monotherapy (ROR: 2.8, 95% CI: 2.5-3.1). Onset time of common endocrinopathies differed between different ICI therapies, typically within 12 weeks in anti-CTLA-4 monotherapy but diffusely ranging from 0 to 48 weeks in anti-PD-1 monotherapy.
Conclusions: Our study shows rising reporting frequencies of endocrinopathies caused by ICIs, especially aggravated in combination therapy. Clinicians should be early aware of latent endocrine toxicity and different onset time of endocrinopathies when implementing ICI therapies.
Keywords: Endocrine toxicity; Endocrinopathy; Immune checkpoint inhibitor; Immune-related adverse event; Onset time.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Brahmer JR, Lacchetti C, Schneider BJ, Atkins MB, Brassil KJ, Caterino JM, et al. Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2018;36:1714–1768. doi: 10.1200/JCO.2017.77.6385. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
