

Racial disparities in peripartum cardiomyopathy: eighteen years of observations
- PMID: 32508175
- PMCID: PMC7719601
- DOI: 10.1080/14767058.2020.1773784
Racial disparities in peripartum cardiomyopathy: eighteen years of observations
Abstract
Background: Black women have greater than a three-fold risk of pregnancy-associated death compared to White women; cardiomyopathy is a leading cause of maternal mortality.
Objectives: This study examined racial disparities in health outcomes among women with peripartum cardiomyopathy.
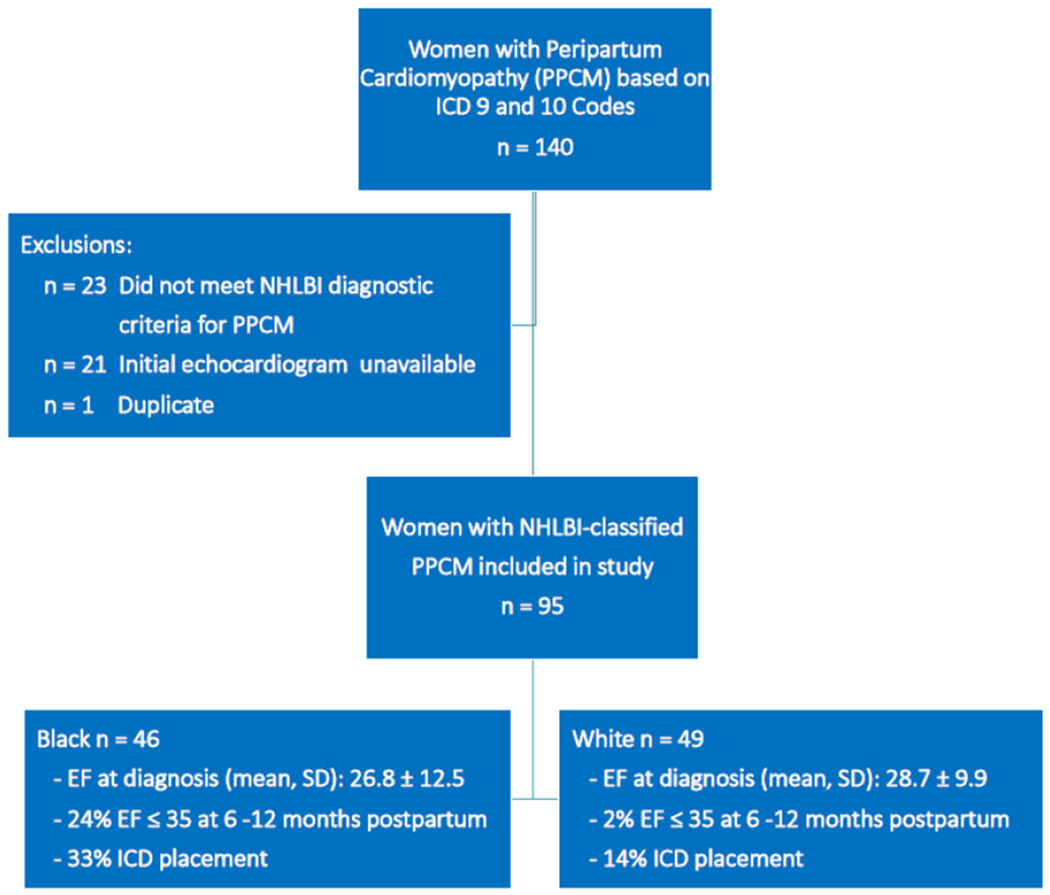
Study design: Retrospective cohort of women with peripartum cardiomyopathy per the National Heart, Lung, and Blood Institute definition from January 2000 to November 2017 from a single referral center. Selected health outcomes among Black and White women were compared; primary outcome was ejection fraction at diagnosis. Secondary outcomes included cardiovascular outcomes, markers of maternal morbidity, resource utilization, and subsequent pregnancy outcomes.
Results: Ninety-five women met inclusion criteria: 48% Black, 52% White. Nearly all peripartum cardiomyopathy diagnoses were postpartum (95.4% Black, 93% White, p=.11). Ejection fraction at diagnosis was not different between Black and White women (26.8 ± 12.5 vs. 28.7 ± 9.9, p=.41). Though non-significant, fewer Black women had myocardial recovery to EF ≥55% (35 vs. 53%, p=.07); however, 11 (24%) of Black women vs. 1 (2%) White woman had an ejection fraction ≤35% at 6-12 months postpartum (p<.01). More Black women underwent implantable cardioverter defibrillator placement: n = 15 (33%) vs. n = 7 (14%), p=.03. Eight women (8.4%) died in the study period, not different by race (p=.48). Black women had higher rates of healthcare utilization. In the subsequent pregnancy, Black women had a lower initial ejection fraction (40 vs. 55%, p=.007) and were less likely to recover postpartum (37.5 vs. 55%, p=.02).
Conclusions: Black and White women have similar mean ejection fraction at diagnosis of peripartum cardiomyopathy, but Black women have more severe left ventricular systolic dysfunction leading to worse outcomes, increased resource use, and lower ejection fraction entering the subsequent pregnancy.
Keywords: Maternal morbidity; maternal mortality; peripartum cardiomyopathy; racial disparities.
Conflict of interest statement
Declaration of Interest Statement
The authors report no conflict of interest.
Figures
References
-
- Harper MA, Meyer RE, Berg CJ. Peripartum cardiomyopathy: population-based birth prevalence and 7-year mortality. Obstetrics and gynecology. 2012. Nov;120(5):1013–9. doi: http://10.1097/AOG.0b013e31826e46a110.1097/aog.0b013e31826e46a1.; eng. - DOI - PubMed
-
- McNamara DM, Elkayam U, Alharethi R, et al. Clinical Outcomes for Peripartum Cardiomyopathy in North America: Results of the IPAC Study (Investigations of Pregnancy-Associated Cardiomyopathy). Journal of the American College of Cardiology. 2015. Aug 25;66(8):905–14. doi: 10.1016/j.jacc.2015.06.1309.. eng. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous