

Inflammatory Cytokines Associate With Neuroimaging After Acute Mild Traumatic Brain Injury
- PMID: 32508732
- PMCID: PMC7248260
- DOI: 10.3389/fneur.2020.00348
Inflammatory Cytokines Associate With Neuroimaging After Acute Mild Traumatic Brain Injury
Abstract
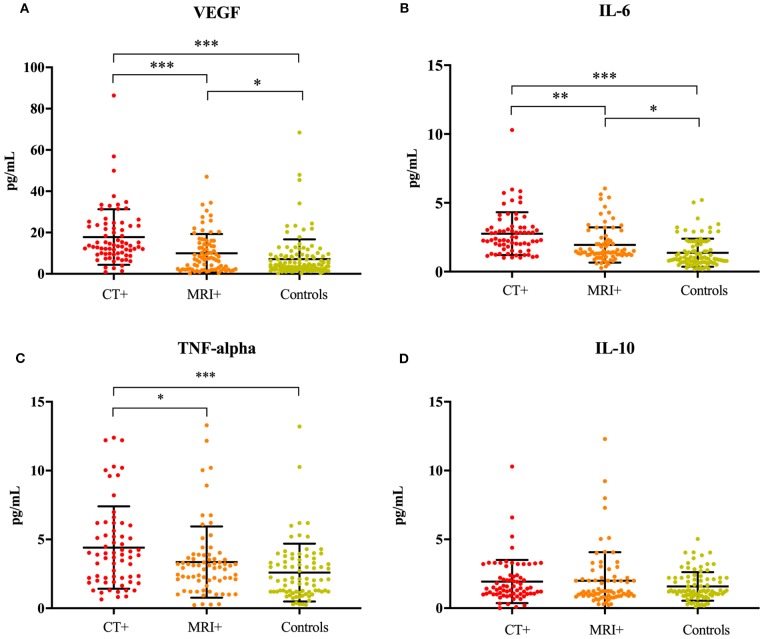
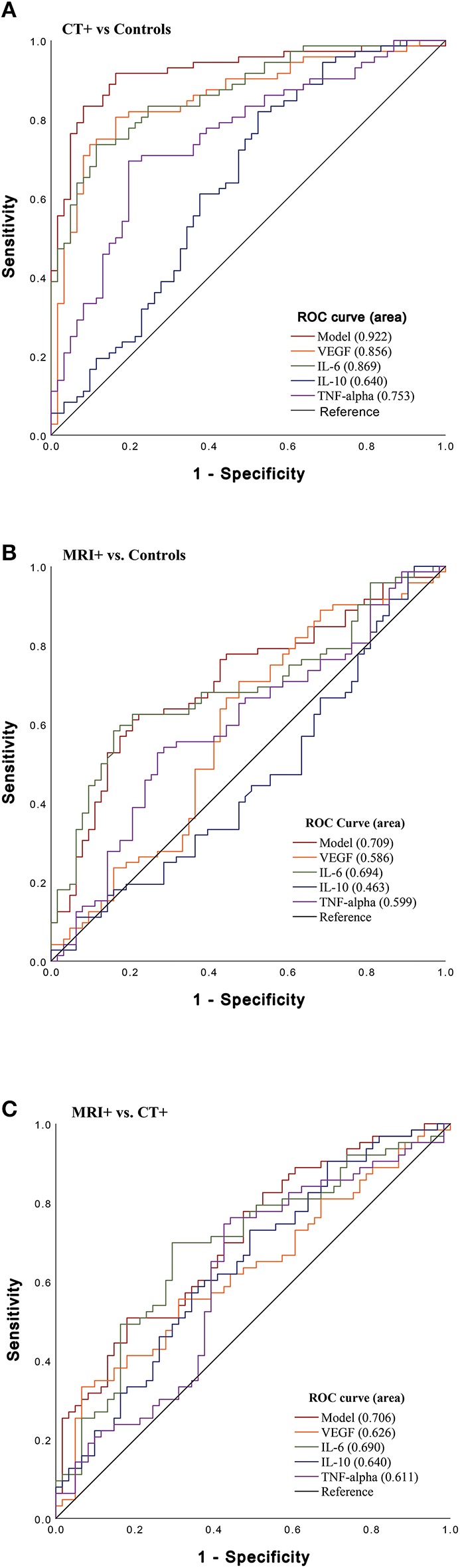
Introduction: Elevated levels of blood-based proinflammatory cytokines are linked to acute moderate to severe traumatic brain injuries (TBIs), yet less is known in acute mild (m)TBI cohorts. The current study examined whether blood-based cytokines can differentiate patients with mTBI, with and without neuroimaging findings (CT and MRI). Material and Methods: Within 24 h of a mTBI, determined by a Glasgow Coma Scale (GCS) between 13 and 15, participants (n = 250) underwent a computed tomography (CT) and magnetic resonance imaging (MRI) scan and provided a blood sample. Participants were classified into three groups according to imaging findings; (1) CT+, (2) MRI+ (CT-), (3) Controls (CT- MRI-). Plasma levels of circulating cytokines (IL-6, IL-10, TNFα), and vascular endothelial growth factor (VEGF) were measured using an ultra-sensitive immunoassay. Results: Concentrations of inflammatory cytokines (IL-6, TNFα) and VEGF were elevated in CT+, as well as MRI+ groups (p < 0.001), compared to controls, even after controlling for age, sex and cardiovascular disease (CVD)-related risk factors; hypertension, and hyperlipidemia. Post-concussive symptoms were associated with imaging groupings, but not inflammatory cytokines in this cohort. Levels of VEGF, IL-6, and TNFα differentiated patients with CT+ findings from controls, with the combined biomarker model (VEGF, IL-6, TNFα, and IL-10) showing good discriminatory power (AUC 0.92, 95% CI 0.87-0.97). IL-6 was a fair predictor of MRI+ findings compared to controls (AUC 0.70, 95% CI 0.60-0.78). Finally, the combined biomarker model discriminated patients with MRI+ from CT+ with an AUC of 0.71 (95% CI 0.62-0.80). Conclusions: When combined, IL-6, TNFα, and VEGF may provide a promising biomarker cytokine panel to differentiate mTBI patients with CT+ imaging vs. controls. Singularly, IL-6 was a fair discriminator between each of the imaging groups. Future research directions may help elucidate mechanisms related to injury severity and potentially, recovery following an mTBI.
Keywords: cardiovascular disease risk; cytokines; inflammation; mild traumatic brain injury; neuroimaging.
Copyright © 2020 Edwards, Pattinson, Guedes, Peyer, Moore, Davis, Devoto, Turtzo, Latour and Gill.
Figures
References
-
- Cassidy JD, Carroll LJ, Peloso PM, Borg J, von Holst H, Holm L, et al. . Incidence, risk factors and prevention of mild traumatic brain injury: results of the WHO Collaborating Centre Task Force on Mild Traumatic Brain Injury. J Rehabil Med. (2004) (43 Suppl):28–60. 10.1080/16501960410023732 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources