

Dendritic Cells and Their Role in Immunotherapy
- PMID: 32508825
- PMCID: PMC7253577
- DOI: 10.3389/fimmu.2020.00924
Dendritic Cells and Their Role in Immunotherapy
Abstract
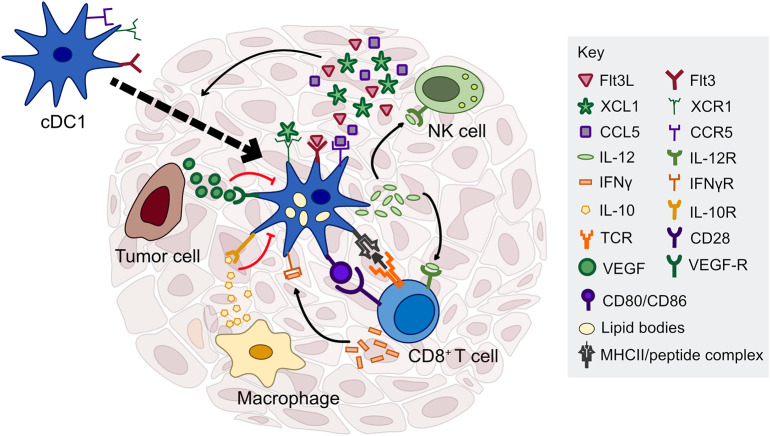
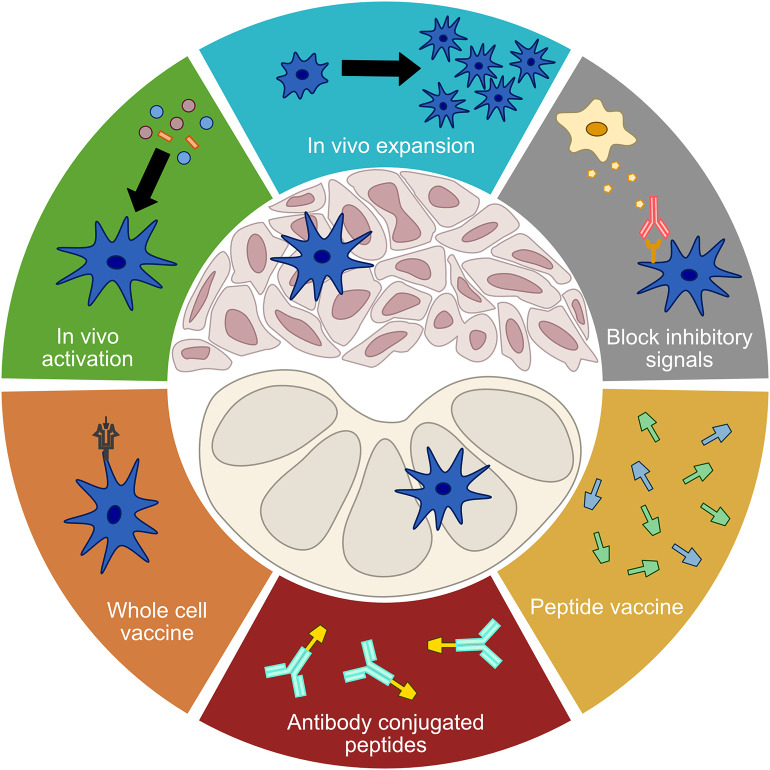
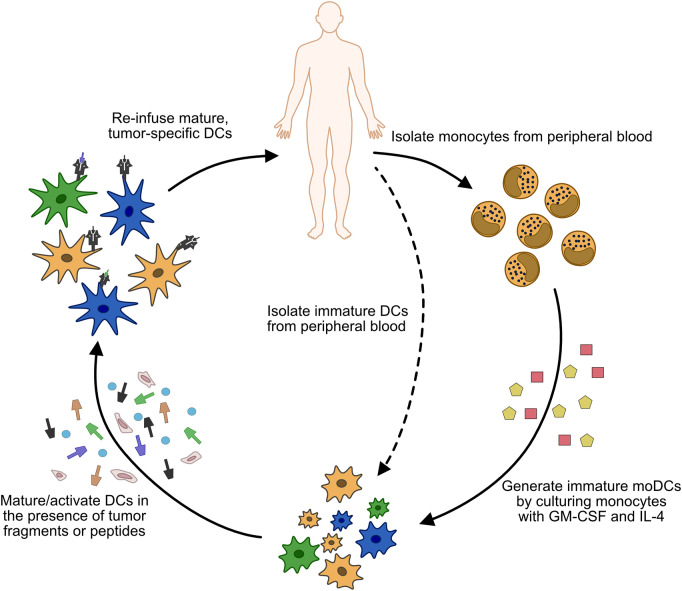
Despite significant advances in the field of cancer immunotherapy, the majority of patients still do not benefit from treatment and must rely on traditional therapies. Dendritic cells have long been a focus of cancer immunotherapy due to their role in inducing protective adaptive immunity, but cancer vaccines have shown limited efficacy in the past. With the advent of immune checkpoint blockade and the ability to identify patient-specific neoantigens, new vaccines, and combinatorial therapies are being evaluated in the clinic. Dendritic cells are also emerging as critical regulators of the immune response within tumors. Understanding how to augment the function of these intratumoral dendritic cells could offer new approaches to enhance immunotherapy, in addition to improving the cytotoxic and targeted therapies that are partially dependent upon a robust immune response for their efficacy. Here we will discuss the role of specific dendritic cell subsets in regulating the anti-tumor immune response, as well as the current status of dendritic cell-based immunotherapies, in order to provide an overview for future lines of research and clinical trials.
Keywords: cancer; dendritic cells; immune checkpoint blockade; immunotherapy; vaccines.
Copyright © 2020 Gardner, de Mingo Pulido and Ruffell.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous