

Short-Term Clinical Outcomes after Using Novel Deeper Intubation Technique (DIT) of Ileus Tube for Acute Bowel Obstruction Patients
- PMID: 32508909
- PMCID: PMC7245673
- DOI: 10.1155/2020/1625154
Short-Term Clinical Outcomes after Using Novel Deeper Intubation Technique (DIT) of Ileus Tube for Acute Bowel Obstruction Patients
Abstract
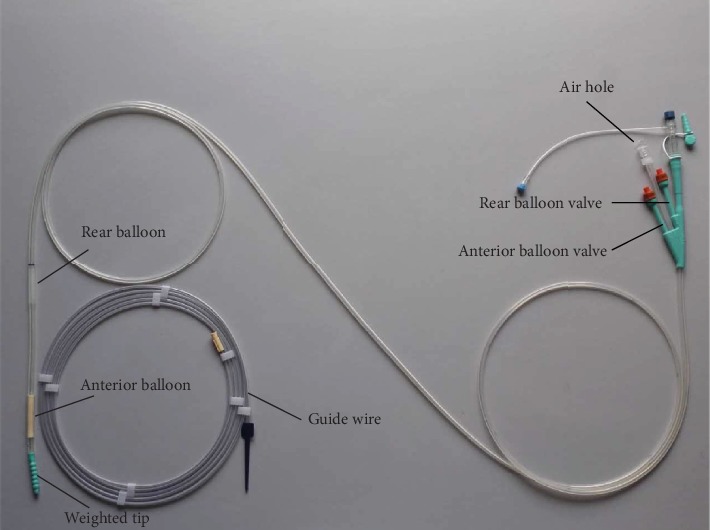
Background: The ileus tube has been widely used for the treatment of acute small bowel obstruction. However, it is difficult to get the tube sufficiently adjacent to the obstruction site due to various reasons.
Methods: We developed a novel intubation technique, named Deeper Intubation Technique (DIT), by using the Zebra Urological Guidewire and digital gastrointestinal fluoroscopy, where we deepened the catheter intubation, and further compared the effects of DIT with the Traditional Intubation Technique (TIT) on the short-term clinical outcomes of 183 patients.
Results: The average intubation depth of DIT apparently exceeds that of TIT (213.89 ± 31.11 vs. 134.67 ± 18.22 cm, P < 0.001). Compared with patients in the TIT group, patients in the DIT group got a lower pain score (P < 0.001), shorter recovery time for anal exhaust defecation (2.87 ± 1.50 vs. 3.37 ± 1.52 d, P = 0.040), higher recovery rate in anal exhaust defecation (24 h, 16.8% vs. 5.7%, P = 0.021; 48 h, 46.3% vs. 27.3%, P = 0.009), better symptomatic remission rate and imaging relief rate (P < 0.05), and increased drainage volume (1006.88 ± 583.45 vs. 821.02 ± 358.73 ml, P = 0.009). Importantly, the emergency surgery rate in the DIT group was lower than that in the TIT group (3.2% vs. 13.6%, P = 0.014). In addition, the DIT procedure was effective for patients with adhesive obstruction but not for cancerous and stercoral bowel obstruction.
Conclusion: Compared to TIT, DIT produced better short-term clinical outcomes, indicating that DIT is a safe and feasible technique for the treatment of adhesive intestinal obstruction.
Copyright © 2020 Yanlu Tan et al.
Conflict of interest statement
The authors declare that there are no conflicts of interest.
Figures
References
-
- Shittu O. B., Gana J. Y., Alawale E. O., Ogundiran T. O. Pattern of mechanical intestinal obstruction in Ibadan: a ten year review. African Journal of Medicine and Medical Sciences. 2001;30(1-2):17–21. - PubMed
LinkOut - more resources
Full Text Sources
