

Towards definitive management of allergic rhinitis: best use of new and established therapies
- PMID: 32508939
- PMCID: PMC7251701
- DOI: 10.1186/s13223-020-00436-y
Towards definitive management of allergic rhinitis: best use of new and established therapies
Abstract
Background: Allergic rhinitis (AR) is an inflammatory disease of the nasal mucosa impacting up to 25% of Canadians. The standard of care for AR includes a treatment plan that takes into account patient preferences, the severity of the disease, and most essentially involves a shared decision-making process between patient and provider.
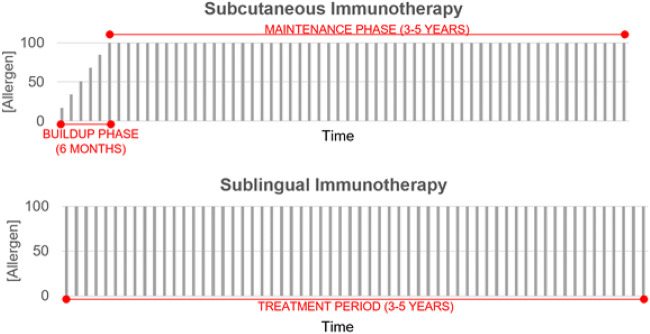
Body: Since their introduction in the 1940s, antihistamines (AHs) have been the most utilized class of medications for the treatment of AR. First-generation AHs are associated with adverse central nervous system (CNS) and anticholinergic side effects. On the market in the 1980s, newer generation AHs have improved safety and efficacy. Compared to antihistamines, intranasal corticosteroids (INCS) have significantly greater efficacy but longer onset of action. Intranasal AH and INCS combinations offer a single medication option that offers broader disease coverage and faster symptom control. However, cost and twice-per-day dosing remain a major limitation. Allergen immunotherapy (AIT) is the only disease-modifying option and can be provided through subcutaneous (SCIT) or sublingual (SLIT) routes. While SCIT has been the definitive management option for many years, SLIT tablets (SLIT-T) have also been proven to be safe and efficacious.
Conclusion: There is a range of available treatment options for AR that reflect the varying disease length and severity. For mild to moderate AR, newer generation AHs should be the first-line treatment, while INCS are mainstay treatments for moderate to severe AR. In patients who do not respond to INCS, a combination of intranasal AH/INCS (AZE/FP) should be considered, assuming that cost is not a limiting factor. While SCIT remains the option with the most available allergens that can be targeted, it has the potential for severe systemic adverse effects and requires weekly visits for administration during the first 4 to 6 months. SLIT-T is a newer approach that provides the ease of being self-administered and presents a reduced risk for systemic reactions. In any case, standard care for AR includes a treatment plan that takes into account disease severity and patient preferences.
Keywords: Allergen-specific immunotherapy; Allergic rhinitis; Antihistamines; Combination therapy; Leukotriene receptor antagonists; Nasal steroids; Pharmacotherapy; Treatment algorithm.
© The Author(s) 2020.
Conflict of interest statement
Competing interestsLH, SL, and SG have no disclosures. AKE has the following disclosures that pose no conflict of interest to the current manuscript. AKE has participated in advisory boards for ALK Abello, AstraZeneca, Aralez, Bausch Health, Circassia Ltd, GlaxoSmithKline, Johnson & Johnson, Merck, Mylan, Novartis, Pediapharm and Pfizer, has been a speaker for ALK, Aralez, AstraZeneca, Boerhinger-Ingelheim, CACME, Meda, Mylan, Merck, Novartis, Pediapharm, Pfizer, The ACADEMY, and Takeda. Her institution has received research grants from Bayer LLC, Circassia Ltd, Green Cross Pharmaceuticals, GlaxoSmithKline, Sun Pharma, Merck, Novartis, Pfizer, Regeneron and Sanofi. She has also served as an independent consultant to Allergy Therapeutics, Bayer LLC, Ora Inc. and Regeneron in the past. The authors declare that they have no competing interests.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
