

Incidence, treatment and mortality of new-onset atrial fibrillation patients at the intensive care unit
- PMID: 32509315
- PMCID: PMC7254104
- DOI: 10.1136/openhrt-2019-001226
Incidence, treatment and mortality of new-onset atrial fibrillation patients at the intensive care unit
Abstract
Objective: Critically ill patients admitted to the intensive care unit (ICU) often develop atrial fibrillation (AF), with an incidence of around 5%. Stroke prevention in AF is well described in clinical guidelines. The extent to which stroke prevention is prescribed to ICU patients with AF is unknown. We aimed to determine the incidence of new-onset AF and describe stroke prevention strategies initiated on the ICU of our teaching hospital. Also, we compared mortality in patients with new-onset AF to critically ill patients with previously diagnosed AF and patients without any AF.
Methods: This study was a retrospective cohort study including all admissions to the ICU of the Martini Hospital (Groningen, The Netherlands) in the period 2011 to 2016. Survival analyses were performed using these real-world data.
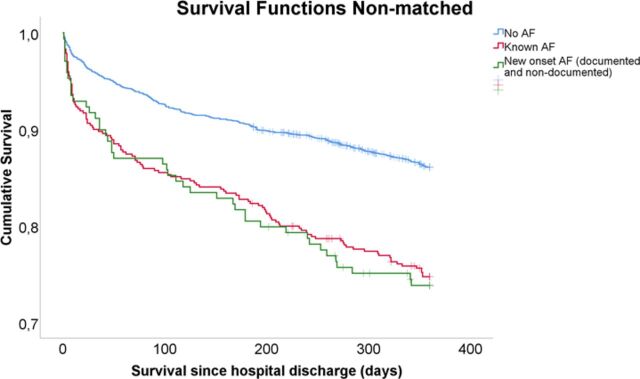
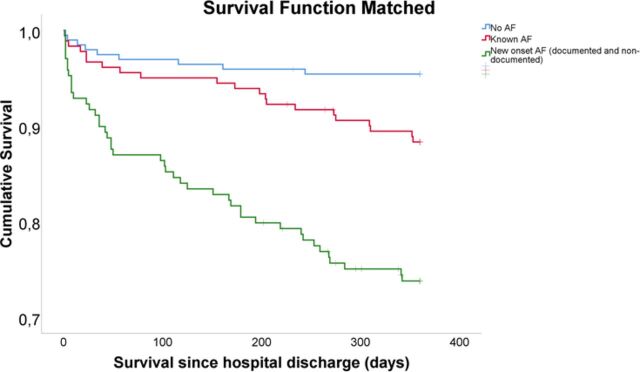
Results: In total, 3334 patients were admitted to the ICU, of whom 213 patients (6.4%) developed new-onset AF. 583 patients (17.5%) had a previous AF diagnosis, the other patients were in sinus rhythm. In-hospital mortality and 1-year mortality after hospital discharge were significantly higher for new-onset AF patients compared with patients with no history of AF or previously diagnosed AF. At hospital discharge, only 56.3% of the new-onset AF-patients eligible for stroke prevention received an anticoagulant. Anticoagulation was not dependent on CHA2DS2-VASc score or other patient characteristics. An effect of anticoagulative status on mortality was not significant.
Conclusion: AF is associated with increased mortality in critically ill patients admitted to the ICU. More guidance is needed to optimise anticoagulant treatment in critically ill new-onset AF patients.
Keywords: anticoagulation; atrial fibrillation; critical illness; mortality; new-onset.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: MJ is an employee of Sanofi. The work presented here is not related to this employment and presents a personal opinion in the context of PhD research. RGT reports grants and personal fees from Boehringer Ingelheim, personal fees from Bayer and personal fees from Pfizer/Bristol Meyer Squibb all outside the submitted work. MJP reports grants and personal fees from various pharmaceutical industries all outside the submitted work. MJP holds stocks in Ingress Health and Pharmacoeconomics Advice Groningen (PAG Ltd).
Figures
Similar articles
-
Incidence, Management, and Associated Clinical Outcomes of New-Onset Atrial Fibrillation Following Transcatheter Aortic Valve Replacement: An Analysis From the STS/ACC TVT Registry.JACC Cardiovasc Interv. 2018 Sep 10;11(17):1746-1756. doi: 10.1016/j.jcin.2018.05.042. JACC Cardiovasc Interv. 2018. PMID: 30190063
-
Stroke prophylaxis in critically-ill patients with new-onset atrial fibrillation.J Thromb Thrombolysis. 2019 Oct;48(3):394-399. doi: 10.1007/s11239-019-01854-5. J Thromb Thrombolysis. 2019. PMID: 30963394
-
Prognosis and management of new-onset atrial fibrillation in critically ill patients.BMC Cardiovasc Disord. 2021 May 5;21(1):231. doi: 10.1186/s12872-021-02039-w. BMC Cardiovasc Disord. 2021. PMID: 33952213 Free PMC article.
-
A Systematic Review of Anticoagulation Strategies for Patients with Atrial Fibrillation in Critical Care.Thromb Haemost. 2021 Dec;121(12):1599-1609. doi: 10.1055/a-1477-3760. Epub 2021 Jun 18. Thromb Haemost. 2021. PMID: 33831963
-
CHA2DS2-VASc Score as Predictor of New-Onset Atrial Fibrillation and Mortality in Critical COVID-19 Patients.J Intensive Care Med. 2024 Nov;39(11):1155-1163. doi: 10.1177/08850666241272068. Epub 2024 Aug 7. J Intensive Care Med. 2024. PMID: 39109625 Review.
Cited by
-
[Atrial fibrillation on the intensive care unit : The special prognostic importance of the first manifestation].Herzschrittmacherther Elektrophysiol. 2022 Dec;33(4):391-397. doi: 10.1007/s00399-022-00899-z. Epub 2022 Sep 26. Herzschrittmacherther Elektrophysiol. 2022. PMID: 36156739 Review. German.
-
Atrial Fibrillation in Critically Ill Patients: Incidence and Outcomes.Cureus. 2024 Feb 28;16(2):e55150. doi: 10.7759/cureus.55150. eCollection 2024 Feb. Cureus. 2024. PMID: 38558719 Free PMC article.
-
Association of Dexmedetomidine With New-Onset Atrial Fibrillation in Patients With Critical Illness.JAMA Netw Open. 2023 Apr 3;6(4):e239955. doi: 10.1001/jamanetworkopen.2023.9955. JAMA Netw Open. 2023. PMID: 37097632 Free PMC article.
-
Automatic Identification of Patients With Unexplained Left Ventricular Hypertrophy in Electronic Health Record Data to Improve Targeted Treatment and Family Screening.Front Cardiovasc Med. 2022 Apr 15;9:768847. doi: 10.3389/fcvm.2022.768847. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35498038 Free PMC article.
-
Atrial fibrillation in critical illness: state of the art.Intensive Care Med. 2025 May;51(5):904-916. doi: 10.1007/s00134-025-07895-0. Epub 2025 May 5. Intensive Care Med. 2025. PMID: 40323451 Review.
References
-
- Lip GYH, Laroche C, Popescu MI, et al. . Improved outcomes with European Society of cardiology guideline-adherent antithrombotic treatment in high-risk patients with atrial fibrillation: a report from the EORP-AF General pilot registry. Europace 2015;17:1777–86.10.1093/europace/euv269 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical