

Thoracolaparoscopic management of a traumatic subacute transdiaphragmatic intercostal hernia. Second case reported
- PMID: 32509954
- PMCID: PMC7264079
- DOI: 10.1016/j.tcr.2020.100314
Thoracolaparoscopic management of a traumatic subacute transdiaphragmatic intercostal hernia. Second case reported
Erratum in
-
Erratum regarding missing patient consent statement in previously published articles.Trauma Case Rep. 2023 Mar 1;45:100808. doi: 10.1016/j.tcr.2023.100808. eCollection 2023 Jun. Trauma Case Rep. 2023. PMID: 37197575 Free PMC article.
Abstract
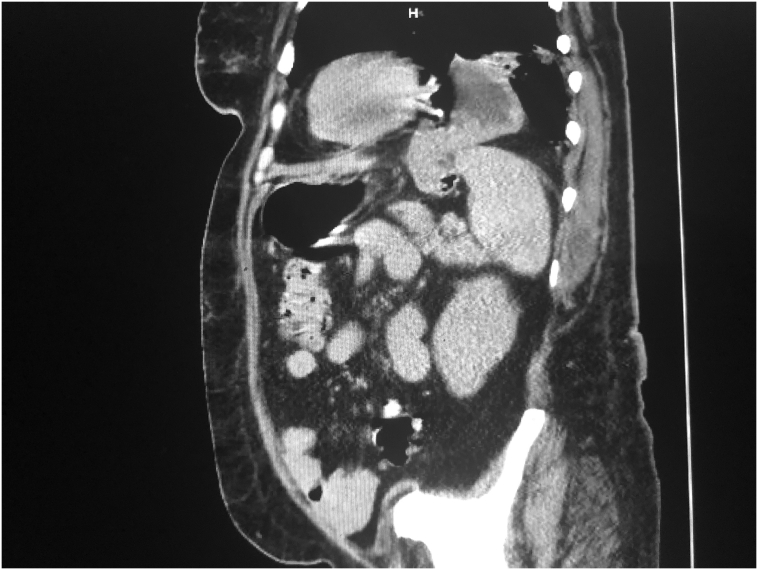
Background: Transdiaphragmatic intercostal hernias are extremely rare. Their physiopathology is different from traumatic diaphragmatic ruptures, and their clinical presentation and management strategies place them in a different category than abdominal intercostal hernias.
Case presentation: A 56 yo female presented to the outpatient trauma clinic with a symptomatic, subacute left sided transdiaphragmatic intercostal hernia secondary to a motor vehicle crash almost 3 months prior to presentation. The injury was managed with a combined thoracoscopic and laparoscopic approach, only the second time ever this has been reported. She was discharged on POD#3, and after 6 months of follow up continues to do well, without clinical evidence of hernia recurrence.
Conclusion: Minimally invasive management of this rare pathology is possible and should be encouraged.
Keywords: Intercostal pleuroperitoneal hernia; Laparoscopic bioprosthetic hernioplasty; TAWH; Transdiaphragmatic intercostal hernia; Traumatic abdominal wall hernia; Traumatic diaphragmatic rupture.
© 2020 The Author.
Conflict of interest statement
None.
Figures





References
Publication types
LinkOut - more resources
Full Text Sources
